JBRA Assist. Reprod. 2016;20 (1):13-16
ORIGINAL ARTICLE
doi: 10.5935/1518-0557.20160004
Low progesterone levels and ovulation by ultrasound assessment in infertile patients
1Federal University of Goiás. Medical School. University Hospital. Gynecology and Obstetrics Department.
Human Reproduction Lab - Goiânia (GO) - Brazil
2Federal University of Goiás – Jataí (GO) - Brazil
CONFLICT OF INTERESTS
No conflict of interest have been declared.
ABSTRACT
Objective:
To assess the correlation between low levels of progesterone and
ovulation by ultrasound monitoring in infertile patients with regular
menstrual cycles.
Methods: Case-control study.
The sample consisted of 302 women aged 20-40 years, treated from 2000
to 2014 in the Human Reproduction Laboratory of the University Hospital
of the Federal University of Goiás and in the Department of Gynecology
and Obstetrics in Goiânia, Goiás. Data collection was performed by
analysis of physical records (Medical Records and Health Information
Services) and electronic ones (Sisfert©, 2004) after approval by a
Human Research Ethics Committee. Patients were classified according to
their ovulatory status, evaluated by progesterone levels and ultrasound
monitoring and divided into two groups: Group I (anovulatory cycle
patients, n=74) and Group II (ovulatory patients, n=228). In both
groups associations were made between the percentage of patients with
normal progesterone (≥ 10 ng/ml) and percentage of patients with low
progesterone (5.65 - 9.9 ng/ml). The groups were paired for comparisons
related to age, body mass index, duration of infertility, follicle
stimulating hormone (FSH), thyroid stimulating hormone (TSH),
luteinizing hormone (LH) and estradiol (E2).
Results:
There was a significant association between the percentage of ovulation
by ultrasound monitoring and the percentages of patients who presented
low levels of progesterone.
Conclusions: The
study suggests that low serum levels of progesterone are associated
with low percentage of ovulation in infertile women with regular
menstrual cycles and women with unexplained infertility.
Keywords: Infertility, Ovulation, Regular cycles, Low progesterone.
INTRODUCTION
The World Health Organization (WHO) defines infertility as the absence
of pregnancy after one year or more of sexual relations with no use of
contraceptives (Rowe et al., 1993).
It is estimated that there are from 50 to 80 million infertile couples
in the world, with about two million new cases per year (Gonçalves, 2005).
This event is experienced by 8-15% of couples in general. In Brazil,
more than 278,000 couples have some difficulty in conceiving a child at
some point in their childbearing age.
The causes of infertility in
women could be due to anatomical factors related to the uterus or the
fallopian tubes; hormonal causes that affect the
hypothalamic-pituitary-ovarian axis; and sterility without apparent
cause (ESCA). It is believed that these factors correspond to 35% of
infertility causes in women, 35% in men; 20% are associated with female
and male issues, and 10% with ESCA.
Ovulatory dysfunctions represent the main causes of female infertility, accounting for up to 40% of them (ASRM, 2012).
Among the causes, hormonal changes are the most important, especially
for infertility. Among them, we can highlight Polycystic Ovarian
Syndrome (PCOS), hypothyroidism, hyperprolactinemia, low levels of
progesterone (P4), among others (McLaren, 2012).
Progesterone (P4) is a hormone produced after puberty, by the corpus
luteum (CL) and by the placenta during the pregnancy and it acts in the
regulation of normal female reproductive functions. The endometrium is
prepared In the womb, facilitating deployment and maintenance of early
pregnancy (Al-Asmakh, 2007).
For this reason P4 plays a vital role in female fertility and low
levels of it can significantly decrease the chances of pregnancy due
the probable influence on endometrial development (ASRM, 2015).
P4 was first associated with the corpus luteum by the huge production
of this steroid after ovulation. Currently, it is known that its
secretion starts from the moment a mature ovarian follicle is
stimulated by LH release (Ke, 2014; Moreira, 2014).
According to the ASRM (2012),
ovulatory function can be evaluated by assessing P4 levels in the
bloodstream, but it should be obtained at appropriate times in the
menstrual cycle.
It is usually recommended that P4 be dosed from 7
to 9 days after the suspected ovulation. Some authors consider this
event to happen with P4 levels starting at 3ng/ml (Guttmacher et al., 1956; Garzia et al., 2004; ASRM, 2012; McLaren, 2012). The World Health Organization (Rowe et al., 1993)
stresses ovulatory P4 levels ≥ 5.65 ng/ml, measured between the 20th
and 24th days of a 28-day cycle. Serum progesterone levels higher than
10 ng/ml are used as a parameter to measure ovulatory function by the ASRM (2012).
P4 levels may suffer discrete increases and cause the non-rupture of a
luteinized follicle (LUF). In this event, the follicle develops itself
normally, grows and matures, but does not break to release the ovum;
however, there may be a P4 secretion, such as a follicle that brakes,
originating the CL. Thus, there is no ovulation, but the follicle
secretes P4, making serum levels increase slightly. In this case,
values don’t reach the 10 ng/ml and it establishes a low level of P4 (Van Zonneveld et al., 1994) causing anovulation.
Low P4 is one of the causes of anovulation and a subtle cause of female infertility (Young & Lessey, 2010),
which can be characterized by insufficient P4 secretion to maintain the
endometrium, preventing implantation and normal embryo growth (Sonntag & Ludwig 2012; Schliep, 2014). It can be found by P4 dosing and through invasive procedures or sophisticated ovulation assessment equipment (Mardesic, 1990).
There’s no standard characterization yet to evaluate progesterone
secretion during the luteal phase in normal fertile women and there is
no established minimum P4 value to determine an adequate luteal
function. Furthermore, it is known that the corpus luteum function
varies from cycle to cycle, but if properly collected, serum
progesterone levels can be useful in clinical diagnosis to assess the
adequacy of the luteal phase (ASRM, 2015).
Some authors suggest that the diagnosis of decreased P4 can be done by levels <10 ng/ml (Van Zonneveld et al., 1994), others indicate values <8 ng/ml (Litwack & Begley, 2001); and Arce et al. (2011)
suggest values between 7.9 - 10 ng/ml may indicate LUF. Although there
is certain proximity between P4 values indicative of LUF, there is
still no consensus about low P4 threshold levels.
The
identification of anovulatory cycles is a challenge for healthcare
professionals. Ovulation prediction or confirmation may also be
obtained by serial monitoring through transvaginal ultrasound, to
measure follicle growth and allow the evaluation of follicular rupture (ASRM, 2012).
Transvaginal US is of the gold standard for ovulation diagnosis during
the menstrual cycle, but difficult to be used in epidemiological
studies. In the absence of this method, measurements of concentrations
of reproductive hormones are commonly used to identify the ovulatory
status in research, among them the measure of P4 levels stands out.
A combination of methods for measuring ovulation has been recommended
in order to obtain a more accurate diagnosis. The Labrep (Human
Reproduction Laboratory) HC/UFG (University Hospital of the Federal
University of Goiás) associates monitoring of ovarian follicles through
ultrasound and the dosage of P4 serum levels to diagnose ovulation,
although women with low P4 are not necessarily submitted to ultrasound
check, which may be responsible for inconsistent ovulatory diagnostics.
This study is justified by the lack of literature showing the low
progesterone influence in the ovulation of infertile women with regular
cycles. Thus, the aim of this study was to evaluate the association
between low levels of P4 and US ovulation assessment in infertile
patients with regular cycles suffering from unexplained infertility.
MATERIALS AND METHODS
This is a
case-control study. There were 302 patients selected, aged between 20
and 40 years, seen between 2000 and 2014 in the Human Reproduction
Laboratory of the University Hospital of the Federal University of
Goiás/UFG and in the Clinic of Gynecology and Obstetrics of the private
healthcare network in Goiania – Goias.
Data was collected from the medical charts stored in the Medical Office
Management System (SAMIS) and from the electronic charts from the
Sisfert© database, which started after approval by the Human Research
Ethics Committee HC/UFG.
Women who had been evaluated by ultrasound and had presented both
regular progesterone levels and ovulatory cycles were included; women
with FSH levels above 9.9 mIU/mL (basal FSH = 1.4 to 9.9 mIU/mL) were
excluded, as were those with TSH higher than 4.7 (basal = 0, 4 and 5
mIU/L) (Garber et al.,
2012), those with Polycystic Ovarian Syndrome with oligomenorrhea or
amenorrhea, users of medicines that would interfere with ovulation and
women under 20 and over 40 years of age.
The patients were broken
down into two groups according to their ovulatory state determined by
transvaginal ultrasound monitoring: Group I (n=74) anovulatory,
comprising women who had P4 levels of 5.65 - 9.9 ng/ml and lack of
follicular collapse - evaluated by monitoring with intravaginal US.
Group II (n=228) ovulatory, consisted of women with P4 levels ≥10 ng/mL
and follicular collapse evaluated by monitoring through US (ASRM, 2012).
Among those groups, two groups were evaluated to obtain the percentage
of patients with normal ovulatory progesterone (≥10 ng/mL) and the
percentage of patients with low progesterone (5.65 to 9.9 ng/mL)
considered as LUF in the study. Those groups were paired for comparison
in relation to age, body mass index, infertility duration, Follicle
Stimulating Hormone - FSH (ng/mL), Thyroid-stimulating Hormone - TSH
(mIU/mL), Luteinizing Hormone - LH (mIU/mL) Estradiol (E2) (pg/mL),
according to Table 1.
The statistical analysis was performed using IBM SPSS Statistics 20.0
(Statistical Packages for Social Sciences, USA) and the Bioestat
(version 5.3). We used the Chi-square test with a confidence interval
of 95% and P
=0.05 for significance level. Where the statistical analysis was not
performed, we calculated the mean value and the standard deviation of
the variables under study.
RESULTS
The results obtained are presented in tables as follows. The comparability of the two populations studied is shown on Table 1. Comparability tests did not show statistically significant differences (P>0.05).
Table 2
shows a significant association between the percentage of ovulation
through ultrasound and the percentage of patients who had low
progesterone levels (OR=0.353); IC (95%): 0.191 – 0.649. P=0.001.
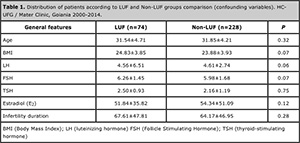
Table 1:
Distribution of patients according to LUF and Non-LUF groups comparison
(confounding variables). HC-UFG / Mater Clinic, Goiania 2000-2014.
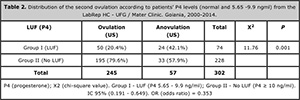
Table 2:
Distribution of the second ovulation according to patients’ P4 levels
(normal and 5.65 -9.9 ngml) from the LabRep HC - UFG / Mater Clinic.
Goiania, 2000-2014.
DISCUSSION
This study has shown that low P4 levels are associated with significant
decreases in ovulation in infertile women with regular cycles, women
with unexplained infertility. This fact was explained by Mesen & Young (2015) when they reported that a defected luteal phase may decrease P4 levels and the fertility in women.
It’s interesting to highlight that, despite the pulsatile release of
P4, its low levels on a single measurement may not always indicate
ovulatory disorders (ASRM, 2012).
On the other hand, this present study found ovulatory changes confirmed
by monitoring through ultrasound in 42.1% of women who presented low P4.
Studies which evaluate P4 values in women with regular cycles are unusual (Fatemi, 2009; Young & Lessey, 2010).
This study evaluated P4 levels in this group of women. While normal P4
values are related to regular cycles and ovulation, lower values may
reflect the presence of unruptured luteinized follicle (LUF) (Schliep, 2014). In a study by Litwack & Begley (2001)
the ovulatory status was evaluated considering the P4 levels for three
menstrual cycles in 543 patients with infertility history longer than
two years. From the population studied so far, 461 (90.2%) had normal
ovulatory cycles confirmed by ultrasound monitoring and 50 (9.8%) had
anovulatory cycles. In this study, values considered suggestive of
ovulation were the ones with P4 levels > 8ng/ml, and P4 levels <8
ng/mL were considered low values. Out of the population being studied,
292 women (63.9%) had normal P4 and 165 (36.1%) had low P4. From the
group with apparently normal P4 values, 7.2% of women got pregnant when
compared to 3.6% of women with low P4. Our study showed significant
reduction (P <0.001) in the fertility of patients with low progesterone levels. It also corroborates the study by Hamilton et al. (1987),
who evaluated 201 ovulatory cycles in 170 infertile women by measuring
ovarian follicles through ultrasound and P4 levels. In our study we
found LUF in 71% of the cycles in which the P4 levels were lower than
10ng/ml, and in 7.9% of cycles in which P4 levels were higher than
10ng/ml. These data corroborate the results of the present study which
also found LUF in cycles (20.4%) in which P4 levels were over 10ng/ml. Eissa et al. (1987)
studied ovulatory cycles in 45 subfertile women and found LUF in 19% of
cycles, but neither reported P4 values used to determine LUF, nor
highlighted the monitoring of the ovulatory follicle through US. The
sensitivity and specificity of diagnostic methods of ovulation were
evaluated by Mesen & Young (2015), wherein they found that P4 levels stand out among other evaluating methods, including endometrial biopsy.
This study showed an association between anovulation through ultrasound and low levels of P4.
CONCLUSIONS
This study suggests that low progesterone levels are associated with a
reduction in ovulation percentage in infertile women with regular
menstrual cycles and women with unexplained infertility. The number (n)
of women used in the study favors greater emphasis on results found.
REFERENCES
Al-Asmakh M. Reproductive function of progesterone. Middle East Fertil Soc. 2007; 12:147-52.
Arce
JC, Balen A, Platteau P, Pettersson G, Andersen A N. Mid-luteal
progesterone concentrations are associated with live birth rates during
ovulation induction. Reprod Biomed Online. 2011; 22:449–56.
Medline Crossref
ASRM
- The Practice Committee of the American Society for Reproductive
Medicine. Diagnostic evaluation of the infertile female: a committee
opinion. Fertil Steril. 2012, 98:302-7.
Medline Crossref
ASRM
- The Practice Committee of the American Society for Reproductive
Medicine. Current clinical irrelevance of luteal phase deficiency: a
committee opinion. Fertil Steril. 2015; 103: 27–32.
Medline Crossref
Eissa
MK, Sawers RS, Docker MF. Characteristics and incidence of
dysfunctional ovulation patterns detected by ultrasound. Fertil Steril.
1987; 4: 603-12.
Medline
Fatemi H M. Assessment of the luteal phase in stimulated and substituted cycles. Facts Views Vis Obgyn. 2009; 1: 30-46.
Medline
Guttmacher AF. Factors affecting normal expectancy of conception. J Am Med Assoc. 1956; 16: 855–64.
Medline
Garzia
E, Borgato S, Cozzi V, Doi P, Bulfamante G, Persani L, Cetin I. Lack of
expression of endometrial prolactin in early implantation failure: a
pilot study. Hum Reprod. 2004; 19:1911–6.
Medline Crossref
Gonçalves J. Avaliação do casal infértil. Rev Port Clin Geral. 2005; 21:493-503.
Link
Hamilton
CJCM, Evers JLH, de Haan J. Ovulatory disturbances in patients with
luteal insufficiency. Clin. Endocrinol. 1987; 26:129–36.
Medline Crossref
Ke, R.W. Endocrine Basis for Recurrent Pregnancy Loss. Obstet Gynecol Clin North Am. 2014; 41:103-12.
Medline Crossref
Litwack G, Begley T, eds. Vitamins and Hormones. Academic Press, San Diego, CA; 2001
Mardesic T. [Unruptured luteinized follicle syndrome]. Zentralbl Gynakol. 1990; 112: 1133-41.
Medline
McLaren JF. Infertility Evaluation. Obstet Gynecol Clin North Am. 2012; 39: 453–63.
Medline Crossref
Mesen
TB, Young SL. Progesterone and the Luteal Phase: A Requisite to
Reproduction. Obstet Gynecol Clin North Am. 2015; 42:135-51
Medline Crossref
Rowe
PJ, Comhaire FH, Hargreave TB, Mellouws HJ. WHO Manual for the
standardized investigation and diagnosis of them infertile couple. New
York. USA. 1993.
Link
Schliep
KC, Mumford SL, Hammoud AO, Stanford JB, Kissell KA, Sjaarda LA,
Perkins NJ, Ahrens KA, Wactawski-Wende J, Mendola P, Schisterman EF.
Luteal phase deficiency in regularly menstruating women: prevalence and
overlap in identification based on clinical and biochemical diagnostic
criteria. J Clin Endocrinol Metab. 2014;99: 1007–14.
Medline Crossref
Sonntag
B, Ludwig M. An integrated view on the luteal phase: diagnosis and
treatment in subfertility. Clin Endocrinol (Oxf). 2012; 77:500–7.
Medline Crossref
Van
Zonneveld P, Te Velde ER, Koppeschaar HPF. Low luteal phase serum
progesterone levels in regularly cycling women are predictive of subtle
ovulation disorders. Gynecol Endocrinol. 1994;8:169-74
Medline Crossref
Young SL, Lessey BA. Progesterone function in human endometrium: clinical perspectives. Semin Reprod Med 2010; 28:5–16
Medline Crossref