JBRA Assist. Reprod. 2021;25(1):81-89
ORIGINAL ARTICLE
doi: 10.5935/1518-0557.20200055
Embryo donation among Latin-Americans who have attended assisted reproduction techniques: a first empirical approach
1Departamento de Atención a la Salud. Universidad Autónoma Metropolitana. Unidad Xochimilco, México
CONFLICT OF INTEREST
The author declares no conflict of interest.
Support
During the study, the researcher received a scholarship from
the National Council of Science and Technology (Consejo Nacional de Ciencia y
Tecnología, CONACYT, Mexico) to conduct doctoral studies at the Complutense
University of Madrid. The research project won the Manuel Velasco Suárez Award
for Excellence in Bioethics 2007 (PAHEF-PAHO/WHO). The first version of this
document received the Mark S. Ehrenreich Prize in Healthcare Ethics Research
2014, through the International Association of Bioethics, and The Pacific Center
for Healthcare Policy and Ethics at the University of Southern California.
ABSTRACT
Objective: To determine whether Latin Americans who have undergone assisted reproduction
techniques would donate embryos.
Methods: This is a multinational cross-sectional study, involving 602 patients. We
invited the Latin American Network of Assisted Reproduction centers. Those
who accepted received the instrument distributed among the patients who
agreed by signing the informed consent form. In total, 261 men and 341 women
participated from seven countries.
Results: Patients would donate their embryos as follows: treatment with embryonic stem
cells (73.6%), heterosexual couples (63.8%), Assisted Reproduction
Techniques (ART) research (57%), scientific or basic research (55.3%),
research with embryonic stem cells (55.2%), premenopausal women (53.8%),
single women (45.1%), people with disabilities (25.4%), lesbians (25.3%),
menopausal women (25.2%), lesbian couples (24.6%), gay couples (19.6%),
senile women (15.1%).
Conclusions: The results favor embryos donation for research purposes, and a little less
for clinical purposes, contrary to what was thought in qualitative studies
conducted among Latin American populations.
Keywords: embryo transfer, embryo destination, embryo research, reproductive techniques, bioethics
INTRODUCTION
The first in vitro fertilization occurred in a physiological cycle. Techno-scientific
approaches hyperstimulated the ovary so that it produced more than one oocyte, thus
increasing the odds of achieving fertilization and implantation, and eventually a
live newborn. Therefore, new medical possibilities and bioethical issues emerged:
oocyte donation, embryo donation, and the possibility of transferring embryos to a
different woman than the one who produced the gamete (surrogacy).
We estimate the need for approximately fifteen oocytes to achieve a live birth (Sunkara et al., 2011). While
obstetric history must be considered clinically (Goldberg et al., 2016); the current trend is the
transfer of a single embryo. The development of vitrification as a cryobiology
technique for the preservation of embryos in a blastocyst reduced the number of
oocytes captured and the number of embryos generated (Liebermann, 2017).
When the “leftover embryos” appeared, they were given several names that do not
necessarily express the same meaning: remnants, supernumeraries, surpluses,
leftovers, spare, unused, unwanted, renounced, unclaimed and abandoned.
Alternatively, the term “embryo donation” became “embryo adoption”, common in the
Christian tradition (Robertson, 2018).
According to the American Society for Reproductive Medicine (ASRM), its use is
inaccurate and not recommended (Ethics Committee of
the ASRM, 2016a). In this study, we used the most accurate concepts of
“remaining embryos” and “embryo donation” (ED). The Latin American Registry of
Assisted Reproduction (RLA) of the Latin American Network of Assisted Reproduction
(REDLARA) only includes the number of embryonic transfers and embryo transfers
originated through oocyte donation, but it does not have data on ED, so that it is
challenging to have quantitative approximations of the phenomenon among Latin
Americans (Zegers-Hochschild et
al., 2019).
ED has reproductive and non-reproductive indications (Dayal, 2013). Among the first are couples with poor prognosis indicators
to achieve pregnancy (ovarian failure, tubal factor, uterine factor, male factor,
carriers of genetic diseases, cancer survivors, failure in previous attempts with
assisted reproduction techniques (ART), and the like). Among the latter, the
economic factor prevailed, since if women only go for embryo transfer, the costs
decrease by at least half; ED is approximately twice as profitable as donating
oocytes, concerning cost per live birth (Finger et al., 2010), and even cheaper than adopting a
child (Gilman & Freivalds, 1997). ED also
provides single women and lesbian couples with an additional opportunity to have
children of their own (Marina et
al., 2010). Another non-reproductive indication has been
research.
Theoretically, there are three possible destinations for remaining fresh embryos:
cryopreserve, discard and donate. Three possible destinations are also available for
the remaining cryopreserved embryos: remaining cryopreserved for own use, discarded
and donated. Therefore, at least two moments are at hand to decide the fate of the
remaining embryos: fresh and cryopreserved. Finally, couples donate their embryos
for the following possible purposes: clinical use (or reproductive use, own use, or
for someone else), research, and education. ED for education (training of clinical
embryologists) is a proposal, even in developed countries.
Research with human embryos generated a growing literature on embryonic stem cells.
In 1998, a group from the University of Wisconsin isolated cells from the internal
embryonic cell mass and developed the first embryonic stem cell lines (Thomson et al., 1998). In
Latin America, the first line of human embryonic stem cells came from Colombia in
2006 (Lucena et al., 2006).
Although research on induced pluripotent stem cells has grown, generating them does
not solve the problem of remaining cryopreserved embryos, since they were generated
in parallel during the process of assisted reproduction.
This study aimed to investigate the opinions for ED in a sample of infertile Latin
American patients in order to obtain information that could be useful for
reproductive medicine centers and the design of ED standards, regulations, or
policies (both ethical and legal), without violating the preferences of couples.
MATERIALS AND METHODS
We contacted and invited REDLARA accredited centers. Those who responded received
complete information about the study (project and instrument). Some members of the
reproductive medicine center team made the personal invitation to participate and
carried out the informed consent process. If patients agreed to participate in the
investigation, they would answer the questionnaire themselves, and after doing so,
they could withdraw their consent, not submitting the completed questionnaire. The
questionnaire was anonymous in order to preserve confidentiality.
This is a cross-sectional, observational, and descriptive study. We created an ad hoc
instrument, consisting of questions used in previous similar surveys found in the
background of this study and relevant for the study, and many other questions were
explicitly created. The first part investigates personal and sociodemographic
background. The second part explores religious beliefs and practices. The third part
includes very brief information on their knowledge about medical history. The fourth
part consisted of opinions towards ED, divided into four subgroups: the feeling of
parenthood, ED for clinical purposes, ED for research purposes, and the importance
of genetic linkage. We used a Likert scale to respond to the statements contained in
the fourth part, where 1 represents “totally agree”, 2 “moderately agree”, 3
“neither agree nor disagree”, 4 “moderately disagree” and 5 “totally disagree”. The
questionnaire had two versions (women and men). For Brazil, we used a certified
translation reviewed by assisted reproduction professionals. The questionnaire also
had information about the study and contact details of the principal
investigator.
The inclusion criteria included: being Latin American by birth, living in a Latin
American country, having already lived at least one cycle with any ART (with or
without pregnancy), and agreeing to sign the informed consent form. There were no
exclusion criteria. The elimination criteria were: being Latin American by birth but
living outside the Latin American region, not being Latin American by birth but
living in Latin America, and submitting an incomplete questionnaire.
The survey registration, statistical processing, and analysis were performed with
SPSS version 16. The study was approved first at the Complutense University of
Madrid, then by the REDLARA Bioethics Interest Group, and finally at each center
that agreed to participate. We considered ethical aspects of the Helsinki
Declaration and the CIOMS Guidelines, because of the international nature of this
study.
RESULTS
In total, 702 patients agreed to participate as research subjects, agreeing to answer
the questionnaire. Once completed, 18 refused to submit it, and 25 of the remaining
ones were eliminated because the respondents were Latin Americans living in a
developed country, 12 were not Latin Americans (in “reproductive tourism” or
“cross-border reproductive care”), and 45 did not respond the questionnaire
completely. Thus, we arrived at 602 research subjects (261 men and 341 women), from
15 reproductive medicine centers in 9 cities (Quito, Salto, La Paz, Lima, Bogotá,
Caracas, Valencia, Ribeirão Preto, and São Paulo) and seven countries (Ecuador,
Uruguay, Bolivia, Peru, Colombia, Venezuela, and Brazil).
Table 1 below summarizes the most relevant
sociodemographic characteristics of the respondents (Table 1). Their mean age was 37.4 years, with a standard deviation of
5.7; 92% were legally married; 67.8% had no children; 34.9% had a bachelor’s degree,
and 25.1% had postgraduate education; 89% identified themselves as part of a
religion; of those who felt part of a religion, 81.7% assumed to belong to the
Catholic Church. Only 31.7% of the participants responded that they had
cryopreserved embryos. The mean response cycle was 2.2, with a standard deviation of
1.4.
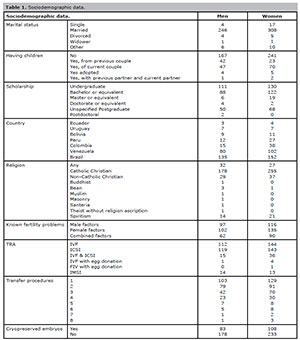
Table 1. Sociodemographic data.
We assessed their feeling of parenthood, that is, the moment in which the participants identified themselves as mothers or fathers. This point provides data on how they understood the status of the embryo. Qualitative data published before this research showed that infertile couples do not have the same considerations about embryo status. They frequently refer to embryos as “children”, even when they are cryopreserved. On the other hand, particularly when they have had negative experiences (no implantation and therefore no pregnancy; spontaneous abortion, and the like), the patients were identified as fathers or mothers at very different times of the assisted reproduction cycle: fertilization (in some centers, biologists comment on how many oocytes were recovered and how many of them were fertilized, and there are even those who allow parents to observe them under the microscope), embryo transfer, with positive pregnancy test, ending the first trimester of pregnancy (in some countries, even fertile women wait for this period to announce the pregnancy to family and friends), until they could see abdominal growth, and those who identified themselves as father or mother later mentioned the birth. No one referred to it after birth. More than half (60.1%) of the research subjects were considered as parents when they received a positive pregnancy test (Table 2).
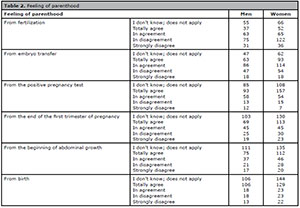
Table 2. Feeling of parenthood
The next section of the instrument analyzes the opinions on ED for clinical purposes (Table 3). The distribution of participants donating their embryos was as follows: 63.8% to heterosexual couples; 53.8% to premenopausal women; 45.1% to single women; 25.4% to people with disabilities, 25.3% to lesbians; 25.2% to menopausal women; 24.6% to lesbian couples; 19.6% to gay couples, and 15.1% to older women.
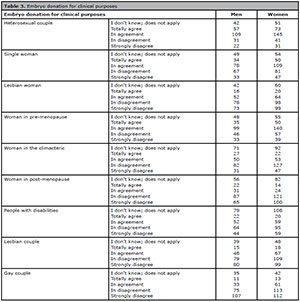
Table 3. Embryo donation for clinical purposes
The next section of the instrument analyzes the opinions on ED for research purposes (Table 4). Participants would donate embryos as follows: 73.6% for stem cell treatments; 57% for ART research; 55.3% for general scientific research; 55.2% for general scientific research; 55.2% for stem cell research; and 55.1% for research that is supervised to ensure it is carried out for the purposes for which they consented.
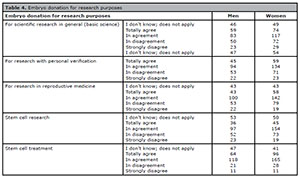
Table 4. Embryo donation for research purposes
DISCUSSION
The issue of embryo status has generated heated debates. Much has been said that it
could be related to religiosity, citing the “Artavia Murillo y otros. (In vitro
fertilization) vs. Costa Rica” case of the Inter-American Court of
Human Rights. The only confessional Central American country, Costa Rica, banned
ARTs. The Court considered that it had violated the human rights of those who sued
the Costa Rican state so that it was requested to pay for damages (Inter-American Court of Human Rights, 2012).
The ruling is also cited in the Province of Buenos Aires, where they recognize
“every human being from the moment of conception” as a “child” (Cámara Nacional de Apelaciones en lo Civil,
1999). Argentinian law used the term “dación de embriones” (from “given
embryo”). However, it is not a purely Latin American issue. In France, one speaks of
“l’accueil d’embryon”, which can be translated as “embryo reception”. However, the
term “accueil” also means “welcoming”, and they do not use the term “donner”
(meaning “donate”; there are no references to the term “don d’embryon”, which would
be the translation to “embryo donation”). This has been interpreted as an
“ultra-early form of adoption” (Malzac,
2011). Besides the ASRM, the European Society for Human Reproduction and
Embryology (ESHRE) also uses and recommends the term “embryo donation” instead of
“embryo adoption” (ESHRE Task Force on Ethics and
Law, 2002).
Despite these and other arguments, the empirical data is inconclusive. Some studies
show an association between religiosity and the possibility of donating embryos
(Mohler-Kuo et al.,
2009), unlike some other studies (Bangsbøll et al., 2004). There was no
statistical association between ED and religiosity in this study. One possible
explanation may be the “popular use of religion” (Rostas & Droogers, 1993). According to these analyses, religious
people express the official position of the Church (mainly Catholic, which does not
officially accept ART; Vatican, 1995), but
reinterpreted with their personal experiences, so they may feel that “God is in the
laboratory” (Roberts, 2006).
The Latin American constant in legal regulation on the subject is the void. However,
it does not also mean that people would not agree to any kind of legal regulation in
place. An example is Sweden, where embryos can be cryopreserved for five years and,
if not claimed, discarded. While ED is not allowed, research shows that both
reproductive medicine professionals (Wånggren et al., 2014) and the general population (Wånggren et al., 2013a; b) would agree with ED. Another example
is Germany, where it is forbidden to generate remaining embryos, donate them, and do
research with them; however, while patients, geneticists and gynecologists would
approve these practices, ethicists would not (Krones et al., 2006).
Opinions about ED for clinical or reproductive purposes show that between one-fifth
and two-thirds are in favor of donating to the different contexts raised in the
instrument. Data in developed countries show that up to 75% agree to donate for
reproductive purposes (Wånggren et
al., 2013a; b). One
possible explanation is that respondents have their own experiences, knowledge, and
understanding of various ART possibilities and are more positive about ED, to help
other infertile couples in their effort to have children (the same project the
participants of this research have or had). Some of the respondents in this study
have been successful with the help of ART, while others have not, and perhaps this
positively affects the response rate, acceptance, and altruistic motive. Some
research has shown that the desire to help others could be significant in ED (McMahon et al., 2003). It is
also notable that those who donate embryos or those who receive them do not see the
procedure as similar to adoption (Millbank et al., 2017).
The least favored option in this investigation was ED to older women, where the women
pregnancy age limit is a controversial issue. The ARTs allowed postmenopausal women
to take on a pregnancy (with oocyte or embryo donation plus hormonal support).
However, the possibility of obstetric complications increases with advanced maternal
age, so that health, in general, and cardiovascular health, in particular, should be
carefully evaluated (MacArthur et
al., 2016). The ASRM recommends deterring women over 55
years of age seeking pregnancy, due to possible complications (Ethics Committee of the ASRM, 2016b).
On the other hand, between a fifth and a quarter of the participants would donate
embryos to gay and lesbian couples. This research shows that if the ED is for single
women, almost half of the respondents would donate embryos, but it falls to half (a
quarter) if the recipients are lesbian. Respondents must consider the possibility of
donating embryos for non-heterosexual people, even if in a low proportion. The LGBT
community is another face of ARTs. The ASRM considers that it is unethical to
prevent access to infertility treatments for single, gay, or lesbian people (Ethics Committee of ASRM, 2013). ESHRE extends
it to gay and lesbian couples and transgender people (De Wert et al., 2014). This data show that
some Latin Americans share liberal and non-discriminatory opinions, such as those of
ASRM and ESHRE. ARTs have increased the classic anthropological discussions about
kinship: family, father, mother, and the like are concepts that have historical and
sociocultural constructions (Álvarez-Díaz,
2014). There are some recent Latin American studies, which analyze the
outcome of children raised by LGTBI parents. It would be useful to educate patients
about this issue, diminish fears and promote understanding (Zegers & Salas, 2014).
Among the most favored options are those associated with research purposes,
especially ED, to achieve stem cell treatments. A systematic review shows that
donating embryos specifically for research ranges from 7% in France to 73% in
Switzerland (Samorinha et al.,
2014). Those who wish to donate embryos usually describe that decision as
better than discarding them; also, they feel reciprocity towards science and
medicine, since they see themselves as recipients of their benefits by having been
able to go to an ART. The review shows that the most important reasons not to donate
were the perception of the risks, conceptualizing the embryo as a person, and lack
of information about the research projects. In this investigation, if the
participants knew the project and had a way to verify it, their response was very
favorable. If we are looking to build public policies and not merely state policies,
we must consult the opinions and suggestions of citizens, where potential donors and
reproductive medicine professionals stand out (Samorinha & Silva, 2016).
The investigation had some limitations. One inherent to reproductive medicine
services in Latin America, because most centers are private, introducing
sociodemographic biases in the sample (economic and educational). Some other
particular limitations are related to areas not included in the instrument used: age
of receiving men, trans people, whether the donation should be anonymous or open,
and the like. The ASRM suggests that the offspring should be informed about their
origin (Ethics Committee of the ASRM, 2018).
Advice to donors, recipients, their families, and the offspring is a crucial issue
(Goedeke et al., 2016).
The data shows that reproductive medicine professionals can instruct their patients
well on the process of a common ART, but little information is managed regarding the
issue of ED (Deniz et al.,
2016).
On the other hand, Latin American countries that consider regulation should have a
general legal framework on ARTs, and something specific that considers ED in
particular. From a purely biomedical perspective, ED is a simple procedure (it
involves embryonic transfer). The difficulty lies mainly in its complex ethical and
legal aspects. It is known, for example, that disputes in cases of divorce or death
of any of the couple members have led to lengthy legal proceedings, among other
things, due to the absence of adequate laws (Cohen
& Adashi, 2016). Some countries restrict or prohibit ED practices,
such as Brazil, Denmark, Israel, Japan, Norway, Sweden, Switzerland, Taiwan, and
Turkey. In other nations, ED is possible under various conditions, such as in
Germany, Australia, Austria, Canada, Spain, U.S., Finland, France, Italy, New
Zealand, and the United Kingdom. The donation practice form also varies
substantially, from anonymous, which has historically been the most common form of
donation, and is allowed in Bulgaria, Denmark, Spain, Greece, India, Portugal, the
Czech Republic, and South Africa; and allowed with varying degrees of open donation.
On the other hand, Canada, Norway, New Zealand, the Netherlands, the United Kingdom,
Sweden, and some states of Australia allow donations in the context of donor
identity registration, where those conceived may access a donation program to know
their genetic information (Goedeke et
al., 2015).
The issue of infertility and ARTs seems to be, at first sight, far from the field of
public health and collective health, and nothing could be farther from the truth in
this case. On the contrary, some issues show techno-scientific tendencies both in
their practice and in reflections from different disciplines. They are part of the
contemporary science and technology agenda, and from the bioethical and political
viewpoint, a challenge concerning equity and justice.
The impossibility of having children has traditionally been seen as a private issue
(Fidler & Bernstein, 1999). However,
public health can contribute significantly by increasing knowledge about
infertility, generating healthcare policies for the reasonable prevention of this
condition, promoting access to medical care that could include ARTs, and, if doing
so, requiring specific regulations. This is even reflected in the specialized
academic publications, where a low representation of the issue of infertility is
evident even in health journals that focus on women (Place et al., 2018).
Two arguments usually emerge when addressing the issue of infertility in less
developed countries: overpopulation, and the limited resources destined for health
care (which they suppose, could not prioritize the issue of infertility, associating
it to ART costs; Ombelet & Goossens, 2017). One should not overlook that it has long been known that
infertility affects globally much less developed countries than developed countries.
While globally estimated at 10% of the world’s population, 80% of infertility is
found in less developed countries (Álvarez-Díaz,
2011). Also, the psychological, social, and economic consequences are
worse for infertile men and women in these countries (Rouchou, 2013).
At first, talking about infertility in less developed countries is indeed a huge
challenge (Asemota & Klatsky, 2015).
However, no one reasonably proposes that ARTs be provided for the entire population.
A first approach, of totally health-related inspiration, is the prevention and
timely diagnosis of conditions that generate infertility (Macaluso et al., 2010). For instance, sexually
transmitted infections are among the leading causes of infertility, especially in
women (Tsevat et al., 2017),
but also in men (Gimenes et al.,
2014). This is because if the healthcare system does not work properly,
these infections may not be diagnosed on time, or are misdiagnosed, or it may be
that they are diagnosed on time and correctly, but an erroneous, suboptimal
treatment is indicated due to a shortage of system resources, or simply the
population does not have the means to pay for the appropriate treatment.
Finally, there is another high-relevance issue: globalization has reached the field
of medical care. Not all countries have the same resources, and within them, not the
entire population has the same economic possibilities. Virtually all Latin American
countries have medical services that provide ARTs (as already stated, they are
mostly private). This causes the emergence of an increasingly studied event: the
so-called “medical tourism” (Álvarez-Díaz,
2012), which in this field is called “reproductive tourism” (although it
is also called “cross-border reproductive care”). This is the reality throughout
Latin America, and was evidenced by discarding several questionnaires precisely
because of this type of population. It is also an urgent call to bioethical and
legal regulations for this event in all countries, since not doing so attaches risks
to public health, problems for international adoptions, and possibility human,
tissue, and cell trafficking (Shalev et
al., 2016). The issue of the possible improper marketing and
cell trafficking has already been raised for ART, concerning oocytes in general
(Neri et al., 2016), or
the investigation of techniques such as mitochondrial replacement (Dickenson, 2013). As far as embryos are
concerned, the possibility of generating markets from the perspective of stem cells
has already been raised (Kahn, 2001), and it
has already been proposed as a possibility for Latin America in the field of ART for
clinical purposes (Álvarez-Díaz, 2005).
This type of research can provide data to analyze from the perspectives of public
healthcare and collective healthcare, not only the issue in the health-disease-care
process, but also the way to address them, generating reflections and arguments that
support the construction of public policies in general, and healthcare policies in
particular. If the issue of infertility and ARTs is viewed from the perspective of
human rights, the purely individualistic vision can be changed, since respecting
sexual and reproductive rights means respecting human rights.
ACKNOWLEDGMENTS
The author is solely responsible for the interpretation of the results. The author
would like to thank Maria Teresa Urbina for her invaluable help and support.
Álvarez-Díaz JA. Una mirada crítica al turismo reproductivo. Salud Problema. 2012;6:36-54.
Asemota OA, Klatsky P. Access to infertility care in the developing
world: the family promotion gap. Semin Reprod Med. 2015;33:17-22.
Medline Crossref
Bangsbøll S, Pinborg A, Yding Andersen C, Nyboe Andersen A.
Patients' attitudes towards donation of surplus cryopreserved embryos for
treatment or research. Hum Reprod. 2004;19:2415-9.
Medline Crossref
Cámara Nacional de Apelaciones en lo Civil. Capital Federal, Ciudad Autónoma de Buenos Aires. Sala I. Rabinovich, Ricardo David s/ medidas precautorias. Sentencia 3 de diciembre de 1999 (cited 2019 Jan 9) Available at: http://www.saij.gob.ar/camara-nacional-apelaciones-civil-nacional-ciudad-autonoma-buenos-aires-rabinovich-ricardo-david-medidas-precautorias-fa99020755-1999-12-03/123456789-557-0209-9ots-eupmocsollaf
Cohen IG, Adashi EY. Embryo disposition disputes: controversies and
case law. Hastings Cent Rep. 2016;46:13-9.
Medline Crossref
De Wert G, Dondorp W, Shenfield F, Barri P, Devroey P, Diedrich K,
Tarlatzis B, Provoost V, Pennings G. ESHRE Task Force on Ethics and Law 23:
medically assisted reproduction in singles, lesbian and gay couples, and
transsexual people. Hum Reprod. 2014;29:1859-65.
Medline Crossref
Deniz SG, Hughes EG, Neal MS, Faghih M, Amin S, Karnis MF. Are
health care providers adequately educating couples for embryo disposition
decisions? Fertil Steril. 2016;105:684-9.
Medline Crossref
Dickenson DL. The commercialization of human eggs in mitochondrial
replacement research. New Bioeth. 2013;19:18-29.
Medline Crossref
ESHRE Task Force on Ethics and Law. III. Gamete and embryo donation.
Hum Reprod. 2002;17:1407-8.
Medline Crossref
Ethics Committee of American Society for Reproductive Medicine.
Access to fertility treatment by gays, lesbians, and unmarried persons: a
committee opinion. Fertil Steril. 2013;100:1524-7.
Medline Crossref
Ethics Committee of the American Society for Reproductive Medicine.
Defining embryo donation: an Ethics Committee opinion. Fertil Steril.
2016a;106:56-8.
Medline Crossref
Ethics Committee of the American Society for Reproductive Medicine.
Oocyte or embryo donation to women of advanced reproductive age: an Ethics
Committee opinion. Fertil Steril. 2016b;106:e3-e7.
Medline Crossref
Ethics Committee of the American Society for Reproductive Medicine.
Informing offspring of their conception by gamete or embryo donation: an Ethics
Committee opinion. Fertil Steril. 2018;109:601-5.
Medline Crossref
Fidler AT, Bernstein J. Infertility: from a personal to a public
health problem. Public Health Rep. 1999;114:494-511.
Medline Crossref
Finger R, Sommerfelt C, Freeman M, Wilson CK, Wade A, Daly D. A
cost-effectiveness comparison of embryo donation with oocyte donation. Fertil
Steril. 2010;93:379-81.
Medline Crossref
Gilman L, Freivalds S. How to realize the joy of adopting a child. Money. 1997;26:160-74.
Gimenes F, Souza RP, Bento JC, Teixeira JJ, Maria-Engler SS, Bonini
MG, Consolaro ME. Male infertility: a public health issue caused by sexually
transmitted pathogens. Nat Rev Urol. 2014;11:672-87.
Medline Crossref
Goedeke S, Daniels K, Thorpe M, Du Preez E. Building extended
families through embryo donation: the experiences of donors and recipients. Hum
Reprod. 2015;30:2340-50.
Medline Crossref
Goedeke S, Daniels K, Thorpe M. Embryo donation and counselling for
the welfare of donors, recipients, their families and children. Hum Reprod.
2016;31:412-8.
Medline Crossref
Inter-American Court of Human Rights (site in the Internet). Artavia Murillo y otros (Fertilización in vitro) Vs. Costa Rica; 2012. Available at: http://www.corteidh.or.cr/cf/Jurisprudencia2/ficha_tecnica.cfm?nId_Ficha=235
Kahn J. Will stem cells create a market for human embryos? J Androl. 2001;22:12. DOI: https://doi.org/10.1002/j.1939-4640.2001.tb02146.x
Krones T, Neuwohner E, Bock K, Manolopoulos K, Tinneberg HR, Richter
G. Attitudes of patients, healthcare professionals and ethicists towards
embryonic stem cell research and donation of gametes and embryos in Germany.
Reprod Biomed Online. 2006;13:607-7.
Medline Crossref
Liebermann J. Human embryo vitrification. Methods Mol Biol.
2017;1568:141-59.
Medline Crossref
Lucena C, Andersson K, Esteban C, Hyllner J, Lucena E. Obtention of
the first Latin American human embryonic stem cell line. Fertil Steril.
2006;86:S510.
Crossref
Macaluso M, Wright-Schnapp TJ, Chandra A, Johnson R, Satterwhite CL,
Pulver A, Berman SM, Wang RY, Farr SL, Pollack LA. A public health focus on
infertility prevention, detection, and management. Fertil Steril.
2010;93:16.e1-10.
Medline Crossref
MacArthur T, Bachmann G, Ayers C. Menopausal women requesting
egg/embryo donation: examining health screening guidelines for assisted
reproductive technology. Menopause. 2016;23:799-802.
Medline Crossref
Malzac P. Enjeux éthiques autour de la question de l’embryon humain. ADSP. 2011;77:28-30.
Marina S, Marina D, Marina F, Fosas N, Galiana N, Jové I. Sharing
motherhood: biological lesbian co-mothers, a new IVF indication. Hum Reprod.
2010;25:938-41.
Medline Crossref
McMahon CA, Gibson FL, Leslie GI, Saunders DM, Porter KA, Tennant
CC. Embryo donation for medical research: attitudes and concerns of potential
donors. Hum Reprod. 2003;18:871-7.
Medline Crossref
Millbank J, Stuhmcke A, Karpin I. Embryo donation and understanding
of kinship: the impact of law and policy. Hum Reprod. 2017;32:133-8.
Medline Crossref
Mohler-Kuo M, Zellweger U, Duran A, Hohl MK, Gutzwiller F, Mutsch M.
Attitudes of couples towards the destination of surplus embryos: results among
couples with cryopreserved embryos in Switzerland. Hum Reprod. 2009;24:1930-8.
Medline Crossref
Neri M, Turillazzi E, Pascale N, Riezzo I, Pomara C. Egg production
and donation: a new frontier in the global landscape of cross-border
reproductive care: ethical concerns. Curr Pharm Biotechnol. 2016;17:316-20.
Medline Crossref
Ombelet W, Goossens J. Global reproductive health - Why do we
persist in neglecting the undeniable problem of childlessness in resource-poor
countries? Facts Views Vis Obgyn. 2017;9:1-3.
Medline
Place JM, Litwack I, Vann S. Is infertility as visible as it needs
to be given its importance to women's health? Results from a review of women's
health journals. Sex Reprod Healthc. 2018;16:80-1.
Medline Crossref
Roberts EF. God's laboratory: religious rationalities and modernity
in Ecuadorian in vitro fertilization. Cult Med Psychiatry. 2006;30:507-36.
Medline Crossref
Robertson CD. Generation, gestation, and birth: An important element
in the embryo adoption debate. Linacre Q. 2018;85:35-48.
Medline Crossref
Rouchou B. Consequences of infertility in developing countries.
Perspect Public Health. 2013;133:174-9.
Medline Crossref
Samorinha C, Pereira M, Machado H, Figueiredo B, Silva S. Factors
associated with the donation and non-donation of embryos for research: a
systematic review. Hum Reprod Update. 2014;20:641-55.
Medline Crossref
Samorinha C, Silva S. A patient-centred approach to embryo donation
for research. Isr J Health Policy Res. 2016;5:44.
Medline Crossref
Shalev C, Moreno A, Eyal H, Leibel M, Schuz R, Eldar-Geva T. Ethics
and regulation of inter-country medically assisted reproduction: a call for
action. Isr J Health Policy Res. 2016;5:59.
Medline Crossref
Sunkara SK, Rittenberg V, Raine-Fenning N, Bhattacharya S, Zamora J,
Coomarasamy A. Association between the number of eggs and live birth in IVF
treatment: an analysis of 400 135 treatment cycles. Hum Reprod. 2011;26:1768-74.
Medline Crossref
Thomson JA, Itskovitz-Eldor J, Shapiro SS, Waknitz MA, Swiergiel JJ,
Marshall VS, Jones JM. Embryonic stem cell lines derived from human blastocysts.
Science. 1998;282:1145-7.
Medline Crossref
Tsevat DG, Wiesenfeld HC, Parks C, Peipert JF. Sexually transmitted
diseases and infertility. Am J Obstet Gynecol. 2017;216:1-9.
Medline Crossref
Vatican. John Paul II. Evangelium Vitae; 1995. Available at: http://w2.vatican.va/content/john-paul-ii/en/encyclicals/documents/hf_jp-ii_enc_25031995_evangelium-vitae.html
Wånggren K, Alden J, Bergh T, Skoog Svanberg A. Attitudes
towards embryo donation among infertile couples with frozen embryos. Hum Reprod.
2013a;28:2432-9.
Medline Crossref
Wånggren K, Prag F, Skoog Svanberg A. Attitudes towards
embryo donation in Swedish women and men of reproductive age. Ups J Med Sci.
2013b;118:187-95.
Medline Crossref
Wånggren K, Baban M, Svanberg AS. Attitudes toward embryo
donation among staff at in vitro fertilization clinics. Acta Obstet Gynecol
Scand. 2014;93:765-70.
Medline Crossref
Zegers F, Salas S, Eds. Bioética, Reproducción y Familia. Santiago: Ediciones UDP; 2014.
Zegers-Hochschild F, Schwarze JE, Crosby JA, Musri C, Urbina MT.
Assisted reproductive techniques in Latin America: The Latin American registry,
2016. JBRA Assist Reprod. 2019;23:255-67.
Medline Crossref