JBRA Assist. Reprod 2006;10(3):19-26
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2006.10.3.04
Laser assisted hatching on frozen-thawed embryos
Assisted hatching com laser em embriões criopreservados
1-Centre for Human Reproduction Prof Franco Junior - Ribeirão Preto, SP, Brazil
ABSTRACT
INTRODUCTION
The objective of the present study was to evaluate the efficacy of quarter-laser zona thinning assisted hatching (qLZT-AH) in improving the implantation rate of cryopreserved-thawed (CT) embryos.
MATERIAL AND METHODS
A total of 258 patients who participated in and ICSI program and had their embryos cryopreserved were divided into two groups: Group I (n = 220), patients who had all their supernumerary embryos cryopreserved, independently of their morphology and Group II (n = 38), patients with risk of ovarian hyperstimulation syndrome (SHO) who had all their embryo cryopreserved. Patients were randomized to be included in the group where qLZT-AH was performed (experimental group) or not (control group) in both population, at the moment of embryo transfer. The population characteristics: age, number of previous transfers, etiology, infertility duration, number of embryo frozen; the embryo factors: survival, cleavage, embryo ZP thickness, embryo quality and the outcomes: implantation and pregnancy rates were evaluated. The transfers were performed by two different protocols: artificial and natural protocols.
RESULTS
Embryo implantation of the hatched embryos did not demonstrated significant difference in relation to the implantation of not hatched embryos in both patients population (Group I: qLZT-AH = 7.8%, Control = 7.9; Group II: qLZT-AH = 28.8%, Control = 14.2% ). The patients who frozen all their embryos (Group II) presented significant higher pregnancy and implantation rates compared to the patients who had exceeding embryos cryopreserved (Group I) (39.5% and 21.3%; 18.2% and 7.8%, respectively). Patients of the Group I who transferred intact embryos in artificial cycles showed higher pregnancy and implantation rates compared to the patients who transferred intact embryos in natural cycles (27.1% and 7.8%; 12.2% and 2.9%, respectively).
CONCLUSION
The present data shown that the qLZT-AH methodology is not efficient to improve implantation rates of cryopreserved embryos.
Palavras chaves: afinamento de uma quarto da zona pelúcida com laser, embriões criopreservados, implantação.
RESUMO
INTRODUÇÃO
O objetivo deste estudo randomizado foi avaliar a eficácia do hatching assistido por afinamento de 1/4 da zona pelúcida (ZP) através de diodo laser na melhora da implantação de embriões congelados e descongelados.
MATERIAL E MÉTODOS
Um total de 258 pacientes que participaram do programa de ICSI e tiveram seus embriões congelados foram distribuídas em dois grupos: Grupo I (n=220), pacientes que congelaram todos os embriões excedentes independente da qualidade embrionária e Grupo II (n=38), pacientes com risco de sindrome de hiperestimualção ovariana (SHO) que congelaram todos os embriões. As pacientes em cada grupo foram randomizadas, para realizar (grupo experimental) ou não (controle) o afinamento de 1/4 da ZP por laser, no momento da transferência. As características das populações: idade, número de ciclos prévios, etiologia, duração da infertilidade, números de embriões congelados; fatores embriológicos : sobrevida, clivagem, espessura da ZP do embrião, qualidade embrionária e resultados: implantação e gravidez foram analisados. As transferências foram realizadas em dois esquemas: ciclo natural e ciclo artificial.
RESULTADOS
A implantação de embriões com ZP afinada por laser não mostrou diferença significativa em relação a implantação dos embriões com ZP intacta em ambos os grupos de pacientes ( grupo I : laser = 7.8% , não laser = 7.9% ; grupo II: laser = 28.8% , não laser = 14.2%). O grupo de pacientes que congelaram todos embriões (Grupo II) obteve maior taxa de gravidez e implantação comparado com o grupo de pacientes que congelaram apenas os embriões excedentes (Grupo I) (39.5% e 21.3% ; 18.2 e 7.8% , respectivamente). Pacientes do grupo I que transferiram embriões intactos em ciclo substitutivo obtiveram maiores taxas de gravidez e implantação comparado com pacientes que transferiram intactos embriões em ciclo natural ( 27.1% e 7.8 % ; 12.2 % e 2.9% , respectivamente).
CONCLUSÃO
O presente estudo demonstra que o método de afinamento de 1/4 da ZP por laser não é eficaz para melhorar a implantação dos embriões criopreservados.
Keywords: quarter laser zona thinning, cryopreserved thawed embryos, implantation
INTRODUCTION
Embryo cryopreservation has been a successful part of assisted reproductive technologies, but the results appear to indicate a reduction in pregnancy and implantation rates compared to fresh embryos. It has been suggested that immersion in cryoprotectants and temperature changes during the process of cryopreservation may affect the physicochemical characteristics of the zona pellucida (ZP) by hardening it and consequently may impair the natural process of blastocyst hatching (Schalkolff et al., 1989; Vicente et al., 1990; Caroll et al.,1990). Assisted hatching (AH) has been used to promote the embryo’s ability to undergo hatching following the cryopreservation procedures (Cohen et al., 1991).
Comparatives studies applying mechanical and chemical AH methodologies to cryopreserved embryos after thawing have been reported to be effective (Tucker et al., 1991, Check et al.,1996, Tao and Tamis.,1997, Vanderzwalmen et al.,2003; Gabrielsen et al.,2004) or not (Edirishinghe et al.,1999) in improving pregnancy and implantation rates. In the last 6 years, the use of non-contact infrared diode laser has become more frequent compared with previous AH methodologies since it allows a rapid, controlled and safe microdissection of the ZP (Rink et al., 1996; Benjamin et al., 2003). Several centers are applying this methodology for AH to fresh embryos and are also using it for embryo biopsies (Veiga et al., 1997; Mantoudis et al., 2001; Baruffi et al.,2000; Petersen et al.,2002; Nagy et al., 2002; Petersen et al., 2005). However, a few randomized studies using laser methodology for cryopreserved-thawed (CT) embryos have failed to show improvement in the implantation rate (Primi et al 2004; Ng et al 2005). The objective of the present study was to evaluate in a randomized manner the implantation and pregnancy rates of CT embryos submitted to quarter-laser zona thinning assisted hatching (qLZT-AH) methodology.
MATERIAL AND METHODS
Patients
The study was conducted on cryopreserved-thawed (CT) embryos from patients who were admitted to an intracytoplasmic sperm injection (ICSI) program. A prospective randomized study of 258 frozen-embryo cycles was performed at the Human Reproduction Center - Prof Franco Junior. According to a protocol approved by the Institutional Ethics Committee, two patient populations were included in this study. Population I: patients who had all their surplus embryos frozen, independently of the embryo morphology (no. of cycles = 220); Population II: patients with risk of ovarian hyperstimulation syndrome (OHSS) who had all of their embryos cryopreserved (no. of cycles = 38).For both populations, whether a patient would be included in the qLZT-AH group or in the control group (no qLZT-AH) was determined by first using a randomized table previously elaborated for the study and then a second randomization by drawing lots at the time the patients were receiving their embryos, i.e. at the time of the transfer cycles. All transfers were performed by a single physician. An identifying code number was assigned to each patient at the time of randomization in order to maintain anonymity.The primary outcome measure was the evaluation of implantation rates and was defined as the number of gestational sacs seen by transvaginal ultrasound examination divided by the total number of embryos transferred. Clinical pregnancy, abortion, and deliveries were calculated for each subgroup in both patients groups (qLZT-AH and control). A pregnancy test was performed on the 14th day after treatment and clinical pregnancy was determined based on the presence of a gestational sac and fetal heart beat by ultrasound scanning 4 weeks after transfer.
ICSI and embryo culture
All patients were submitted to the routine scheme of controlled ovarian stimulation (Franco Jr et al, 2001). Oocyte retrieval was performed 36 hours after hCG by transvaginal ultrasound-guided aspiration. ICSI was performed according to the method of Svalander et al (1995). Oocytes were examined after 17-20 hours to assess fertilization and those with two distinct pronuclei were considered to be normal zygotes. Twenty-five to 27 hours after injection, on the 1st day of culture, early cleavage was evaluated and 2-cell embryos were separated for transfer (Petersen et al., 2001). For population I, embryo transfers were carried out on day 2 or day 3, according to the number of 4-cell embryo stages with equal regular blastomeres (grade I embryo) available on day 2. Day 2 embryo transfers were performed when = 3 grade I embryos were available on day 2. On the other hand, if > 3 grade I were available on day 2, embryo transfers were carried out on day 3 in other to enhance embryo selection. However, for population II, all fresh embryos were cryopreserved on day 2.
Freezing procedure
Embryo cryopreservation was performed using a freezing media kit (Irvine Scientific, USA) which contained the following solutions: PBS, 1.5 M propanediol (PROH) and 1.5 M PROH + 0.1 M sucrose. The material was cooled in a programmable freezer (Cryologic CL-863, Australia) with a starting temperature of 24oC. Cooling rate was 2oC per minute until -6oC, when manual seeding was performed. The temperature was then reduced 0.3oC per minute until -35oC, followed by a free fall to -150oC, after which the straws were transferred to liquid nitrogen.
Thawing procedure
For the thawing process, an embryo thaw media kit (Irvine Scientific) was used. Embryos were thawed by removing the straw from storage, exposure to air for 30 s and immersion in a water bath at 30ºC for 40 s. The embryos were successively added to different PROH solutions (1.0 M PROH/0.2 M sucrose, 5 min; 0.5 M PROH/0.2 M sucrose, 5 min) followed by 0.2 M sucrose for 10 min. Rehydration was completed by transferring the embryos to PBS medium for 5 min at room temperature and to PBS stabilized at 37oC in the presence of 5% CO2 for a further 5 minutes (Mauri et al., 2001). The criterion for the evaluation of morphological survival was that the thawed embryo would have at least one intact blastomere and no signs of damage to the zona pellucida (Lai et al., 1996). Surviving embryos were transferred to 50 µl microdroplets of P1/10% HSA or blastocyst medium/10%HSA (Irvine Scientific) in falcon dishes, depending on the day they were frozen, and were placed in culture for 24 hours at 37ºC/5.5%CO2. Frozenthawed embryo transfer was performed after assessment of embryo cleavage, when the division of at least one of the blastomeres was observed after 24 hours of culture (Van der Elst et al., 1997). Embryos that presented a continuation of the embryo cleavage process were preferentially transferred. However, when it was not available, embryos with no continuation of the cleavage were also transferred. On the other hand, exceeding cleavage embryos were leave in culture and refrozen in a blastocyst stage when available.Embryo quality was assessed at the time of transfer for all patients according to the following criteria: grade 1, embryos with 8 cells by day 3 or the morula stage by day 4 without fragmentation and with all their blastomeres intact after thawing; grade 2, embryos without 8 cells by day 3 and/or no morula stage by day 4 with =25% of their blastomeres intact after thawing and/or with =25% fragmentation; grade 3, embryos without 8 cells by day 3 or no morula stage by day 4 with >25% of their blastomere intact after thawing and/or >25% fragmentation.
Transfer cycles
Two different protocols were used for transfer:
In the natural cycle, follicular development was monitored by serial vaginal ultrasonography starting on the 10th day of the cycle. A 10000 IU dose of hCG was administered when a follicle of > 17 mm was observed. Thawing was routinely performed on the fifth or sixth day after hCG (day of hCG injection = day 0) and embryos were transferred on the sixth or seventh day after hCG, depending on the day on which they were frozen.
In the artificial cycle, estradiol valerate (Postoval, Wyeth, São Paulo, SP, Brazil) was administered from the first to the 14th day of the cycle at a daily dose of 6 mg. Progesterone (Utrogestan, Besins International, France) was also introduced on the 14th day at a dose of 400 mg/day by the vaginal route, as long as endometrial thickness was > 6 mm (Oliveira et al., 1997) and was increased to a daily dose of 800 mg on the day of embryo transfer. Thawing was performed on the fifth or sixth day of progesterone treatment and embryos were transferred on the sixth or seventh day, depending on the day on which they were frozen.
Assisted hatching procedure
The embryos were positioned for the assessment of ZP thickness before laser manipulation and transfer. ZP thickness measurements were performed at four points (9, 12, 3 and 6 o’clock positions), using an inverted Eclipse TE 300 microscope (Nikon Instrument, NY, USA) equipped with a Hoffman lens and an ocular micrometer. qLZT-AH was performed with a 1.48 µm wavelength (infrared) diode laser (FertilaseTM system, Medical Technologies Montreux, Lausanne, Switzerland) with a pilot laser light that operated through a 40x microscope objective mounted on an inverted Eclipse TE 300 microscope with displacement heated stage. The embryos were treated directly in their original dish containing 50 µl microdroplets of culture medium, a Falcon 1006 Petri dish (Becton Dickinson, Denmark). qLZT-AH was performed by thinning the ZP to a depth of 50-80% of its thickness starting at one point and continuing until 25% of the ZP was irradiated, i.e. laser thinning was initiated at the 9 o’clock position and consecutive irradiations were generated until the 12 o’clock position, with an irradiation time of 9 ms to reach a total length of approximately 80 µm.
Data Analysis
Data are reported as means ± standard deviation and were analyzed using the InStat 3.0 program for Macintosh (GraphPad Software, San Diego, CA, USA). The Mann-Whitney test and Fisher exact test were used when appropriate. The level of significance was set at p<0.05.
RESULTS
A total of 350 laser-thinned CT embryos were compared with 352 intact CT embryos. The patient characteristics such as age at embryo freezing, age at embryo thawing, infertility duration, primary and secondary infertility, etiology, number of cycles, number of frozen embryos, number of previous transfers did not differ between the qLZT-AH and control groups or between populations I and II (Tables 1 and 2, respectively).
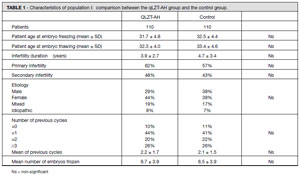
TABLE 1. Characteristics of population I: comparison between the qLZT-AH group and the control group.
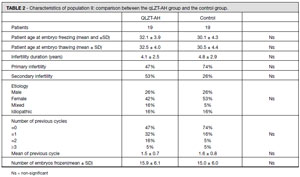
TABLE 2. Characteristics of population II: comparison between the qLZT-AH group and the control group.
Embryo factors such as survival and cleavage rates of CT embryos, mean number of embryo transferred and ZP thickness were the same for the qLZT-AH and control groups and for population I and II (Tables 3 and 4, respectively).
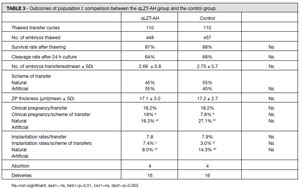
TABLE 3. Outcomes of population I: comparison between the qLZT-AH group and the control group.
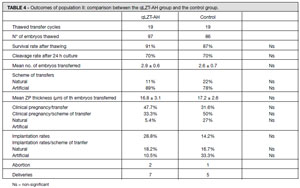
TABLE 4. Outcomes of population II: comparison between the qLZT-AH group and the control group.
For Population I, a total of 20 clinical pregnancies (18.2%) and an implantation rate of 7.8% were achieved with the use of AH. This did not differ from the control group in which the thawed embryos were transferred with an intact zona (18.2%% and 7.9%, respectively) (Table 3).
However, for population II, more patients achieved pregnancy when qLZT-AH was applied, although the rate was not statistically different from the control group (47.4% and 31.6%, respectively). We also observed a higher implantation rate for laser-thinned embryos compared to control, but without statistical significance (28.8% and 14.2%, respectively) (Table 4). Deliveries and abortions were similar for the qLZT-AH and control groups and for both populations.
Embryo quality after thawing was evaluated in both populations. Figures 1 and 2 show the percentage of grade 1, grade 2 and grade 3 embryos in population I and population II, respectively. No significant difference was observed between the qLZT-AH and control groups.
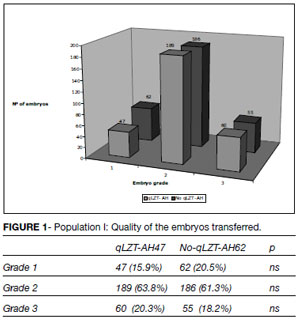
FIGURE 1. Population I: Quality of the embryos transferred.
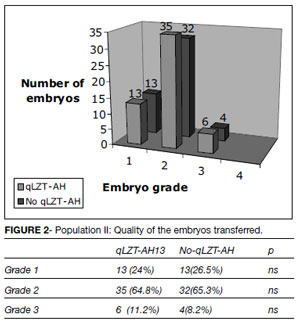
FIGURE 2. Population II: Quality of the embryos transferred.
Two different schemes of transfer (natural and artificial) were used for both the qLZT-AH and control groups and both populations (I and II). In population I of the control group, more pregnancies were achieved when the embryos were transferred in an artificial cycle (27.1%) compared with natural cycles (7.8%), (p<0.05). However, this significant difference was not observed in the qLZT-AH group. In population II there was not difference in implantation pregnancy rate between the laser and control subgroup either for artificial or natural transfer cycles (Table 3).
DISCUSSION
One of the reasons that have been suggested to explain the general lower implantation rates after transfer of CT embryos compared with fresh embryos is the alterations that occur in the glycoprotein matrix (zona pellucida) during the freezingthawing process, causing the embryo to have ‘exacerbated abnormal zona hardness’ which results in failure of embryonic zona pellucida rupture, a prerequisite for implantation (Cohen et al., 1991, Tucker et al., 1991). AH has been used as a method for improving the implantation potential of these CT embryos with a ‘harder zona’ since it may improve the chances of the embryo attaching to the womb by allowing earlier contact and dialogue between the embryo and the endometrium.
Conflicting information regarding the impact of AH on CT embryos exists in the literature. AH in CT human IVF embryos was first performed mechanically by Tucker et al, (1991) who reported a trend towards an improved implantation rate with the use of the partial ZP dissection methodology. Other groups later showed that chemical AH using acidic Tyrode solution is an effective method for the improvement of implantation and pregnancy rates in thawed embryo transfers (Check et al., 1996; Tao and Tamis, 1997 and Gabrielsen et al., 2004).
In contrast to the chemical AH method, for which only beneficial effects have been demonstrated, the effect of mechanical hatching on CT embryos has been reported to be beneficial (Vanderzwalmen et al., 2003) or not (Edirisinghe et al., 1999).
On the other hand, AH laser methodology has been successfully applied for the last decade in fresh embryo transfers (Antinori et al., 1996; Petersen et al., 2005). It permits a controlled and rapid microdissection of the ZP and its safety has been proved in both animals (Germond et al.,1995) and humans (Germond et al., 2000). Laser irradiation produces photolytic ablation of the ZP without alteration of the cytoplasmic structure. Although it has been much applied to fresh embryos, its use for CT embryos has been described only in the last two years in two reports (Primi et al., 2004 and Ng et al., 2005).
Primi et al. (2004), in a multicenter study, were the first to perform AH with a diode laser in CT embryos. The study was carried out at four IVF centers in which AH was performed on 405 embryos by opening their ZP in a single breach in patients coming for the first or third transfer cycle of CT embryos. For patients undergoing their first CT embryo transfer cycle, significantly lower pregnancy (1.6 x 15.1%;p=0.01) and implantation (1.6% x 10%;p=0.01) rates were obtained when they received laser-drilled embryos and no immunosuppressive/antibiotic treatment compared to control. In addition, patients coming for the third transfer cycle did not benefit from the use of laser methodology
Recently, Ng et al. (2005), in a randomized study using the same methodology as used in our study, did not show improvement in implantation or pregnancy rates after transferring 188 laserthinned CT embryos (9.0% and 12.5%, respectively) compared to control (6.8% and 15%, respectively), suggesting that laser AH should not be performed routinely in all CT embryos.
The data obtained in this prospective and randomized study failed to show a significant improvement in the implantation rate of CT embryos after using the qLZT-AH methodology in patients who had their surplus or all embryos cryopreserved. The present study agrees with the two previous studies using laser methodology. However, both previous studies showed an important bias that could affect the interpretation of the outcomes. In the study of Primi et al (2004), patients submitted to pseudo-randomization based on historical control were used as control for the group of patients who were coming for the third transfer.
Furthermore, in the report of Ng et al (2005) the randomization was not efficient in producing two groups (AH and control) with similar numbers of embryos transferred, suggesting that the clinical criteria defining the number of embryos to be transferred were not the same for the AH and control groups. Thus, both the historical control group (Primi et al., 2004) and the imbalance in embryo number (Ng et al., 2005) could affect the interpretation of the outcomes.
The quality of the embryo is a factor that can affect the outcomes. To freeze all of the exceeding embryos independently of their morphology is an important factor that should be considered in evaluating the results. In Brazil, it is not permitted to discard poor quality embryos and to freeze them could impair the results.
For this reason, the quality of the CT embryos transferred was evaluated in both populations. Our data showed no significant difference in the quality distribution of CT embryos (grades I, II and III) in the qLZT-AH and control subgroups for either population I or II. Patients of population I received 16% and 20.4% of grade I CT embryos in the qLZ-AH and control groups, respectively, and patients of population II received 24% and 26.5% of grade I CT embryos in the qLZT-AH and control groups, respectively.
CT embryo transfers have been successfully performed in natural cycles following spontaneous ovulation and in cycles in which the endometrium is artificially prepared with exogenous steroids. Studies in the literature have compared the outcome of natural CT embryo transfers to artificial cycles, with conflicting results. Some groups have shown no difference in pregnancy rates using or not artificial cycles (Sathanantam et al., 1991; Al-Shawaf et al., 1993; Gelbaya et al 2006), while others have shown higher clinical pregnancy rates in women who underwent artificial CT embryo transfer cycles (Schmidt et al., 1989; Muasher et al., 1991; Davies et al., 1991).
In our study, for those patients who had their exceeding embryos cryopreserved a significantly higher pregnancy and implantation rate was obtained in artificial transfer cycles compared to natural transfers (27.1% x 7.8% and 12.2% x 2.9%, respectively, p<0.05) when control CT embryos were transferred. The same was not observed for the qLZT-AH group, for which the pregnancy and implantation rates were similar for artificial and natural transfer cycles (18.3% x 8.0% and 18% x 7.4%, respectively), showing no effects on outcomes with the use of qLZT-AH and artificial transfer cycles for this specific subgroup. For patients who froze all their embryos, the data showed no difference in outcome between artificial and natural cycles but the number of transfers in natural cycles were too small to permit any conclusion.
On the other hand, pregnancy and implantation rates were statistically different between populations I and II. Patients who froze all their embryos showed significant higher implantation (p=0.005) and pregnancy (p=0.0001) rates compared to patients who had only exceeding embryos cryopreserved (39.5% and 21.3%; 18.2% and 7.8%, respectively).
One interpretation for this fact could be the large number of oocytes collected from this population, making this population favorable. In addition, in population II there was a high incidence of patients with chronic anovulation and 83% of the transfers of this population had to be performed in artificial schemes. This fact may also have helped improve the results for this specific population, at least for the control group.
In the literature, few randomized studies evaluating the efficacy of qLZT-AH on CT embryos with a large number of data are available. There is only one study assessing a total of 188 CT embryos. Our data show the results of 350 microdissected embryos and can be helpful to evaluate the real efficacy of qLZT-AH for CT embryos.
In conclusion, qLZT-AH was not efficient regarding CT embryo cleavage either for patients who had supernumerary embryos or for those with all their embryos cryopreserved and should no be routinely used in an IVF program for cryopreserved embryos.