JBRA Assist. Reprod. 2008;12(2):14-18
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2008.12.2.03
Incidence of male infertility by occupational factors In the State of Minas Gerais
Incidência da infertilidade masculina por fatores ocupacionais no Estado de Minas Gerais
*PhD. Institute of Biological Sciences (ICBS), Pontifical Catholic University of Minas Gerais, Email:taitson@pucminas.br
**PhD. Institute of Gynecology (IG), Federal University of Rio de Janeiro (UFRJ)/ G&O Barra-RJ. Av das Américas 4666 salas 312-313, Barra da Tijuca, Rio de Janeiro, RJ. Brasil. Cep 22649-900. Phone-55-21-2430-9060; Fax 55-21-2430-9070, Email: mariadocarmo@cmb.com.br
Abstract
Objective: The occupational factors are defined in the etiology of male infertility.
Methods and results: This study was designed from the authors` database regarding 24.280 infertile men. 102 individuals (0,42%) were estimated for this set of causes. The professionals that work in X - ray services, 79 individuals (77,46%), were the most relevant finding. The cause of infertility in 15 men was the exposure to organochlorine insecticides. Three cases of infertility (2,94%) were reported in workers in the lead industry. The same number of cases and the same incidence (2,94%) were found in workers in precious stones mining, due to mercury handling. The exposure to cadmium and copper were able to generate infertility in one individual each (0, 98%).
Conclusion: The expressive sampling of etiologies in male infertility by occupational factors in the area studied (102) and the number of municipal districts where the datum was collected (27 districts), associated to the clinical conditions, qualify these etiologies as predictive-evolutionary markers of reproductive health in the state of Minas Gerais - Brazil - similar to what takes place with populations in other parts of the world.
Key words: environment, infertility, male infertility, occupational factors, epidemiologic studies
Resumo
Objetivo: Fatores ocupacionais são hoje bem definidos na etiologia da infertilidade masculina.
Métodos e resultados: Os dados deste estudo foram obtidos da casuística dos autores, relacionados a 24. 280 homens inférteis. Destes, 102 indivíduos (0,42%) foram identificados para esta etiologia. O achado mais relevante relacionou-se com os profissionais que trabalham com raios X (77,46%), seguidos de 15 exposições a inseticidas organoclorados. Houve 3 casos (2,94%) relacionados a trabalhadores da indústria do chumbo. O mesmo número e a mesma incidência foi registrado em trabalhadores de minas de pedras preciosas, devido à manipulação de mercúrio. A exposição ao cádmio e ao cobre causaram infertilidade em 1 caso cada (0,98%).
Conclusão: A expressiva amostragem das etiologias da infertilidade masculina por fatores ocupacionais observada nesta casuística de localização geográfica definida (102) e o número de municípios em que o dado foi constatado (27 municípios), associados às condições clínicas, qualificam estas etiologias como marcadores preditivo-evolutivos de saúde reprodutiva no estado das Minas Gerais, à semelhança do que ocorre com populações de outras partes do mundo.
Palavras-chave: meio ambiente, infertilidade, infertilidade masculina, fatores ocupacionais, estudos epidemiológicos.
INTRODUCTION
Infertility is the inability or the reduced ability to achieve pregnancy, without using contraceptive methods, in a 12-month period. Nearly 50% of the couples conceive the first pregnancy in the first 3-5 months and 85% up to 12 months. In a subsequent pregnancy they have the following rates: 33% for the first month and 50% for two months. Out of these couples, 15% cannot get pregnant in a year, which defines the percentage of infertile couples (Greenhall et al., 1990; Irvine, 1998).
The occupational factors are well defined as one of the causes of male infertility. Significant associations were found when comparing the seminal parameter of individuals exposed to chemical substances, such as mercury, pesticides and estrogens. Psychological stress also proved to be another important factor for infertility. Other works already show the negative impact of stress in the seminal parameters. Thus, more and more, the occupational factor (work) appears as an important cause of male infertility (Sheiner et al., 2003).
The environment has the capacity of acting in different ways in male fertility. Each isolated causal factor is able to provoke different levels of commitment, either in the production of spermatozoa, sexual inadequacy, libido or even hormonal levels. The environmental hazards many times able to change the fertility in man are excessive heat, electromagnetic radiation and heavy metals. (Robaire et al., 1995; Orejuela et al., 1998).
Harmful effects in fertility have been observed in men routinely exposed to environments with excessive heat. Under normal conditions, the testicle acts as a system of thermoregulation, keeping the scrotal temperature at an average two degrees below body temperature. Professional drivers and particularly workers constantly exposed to high temperatures may develop the difficulty of keeping intratesticular temperature low (Thonneau et al., 1998). The action of chemical substances in the organism, such as gonad toxics, is linked to concentration, cumulative effect (low or partial excretion), duration of exposure, doses-effect relation and metabolism. In some cases the effects are reversible, but in others they are not. The main citotoxic drugs that inhibit the spermatogenesis are cisplatine, busulfan, cyclophosphamide, chlorambucil, methotrexate and vincristine.
Although the ionizing radiations have a more discreet effect on the already differentiated cells, irradiated spermatozoa are usually unable to fertilize, due to the alteration in the chromatin. In turn, the mother cell of the spermatozoa (spermatogonia) is less sensitive to the action of radiations. After the irradiation, the testicles may need several years for the restoration of the germinative epithelium. Therefore, the professionals that work in this area (radiologists and radioactive material operators) may have their testicular function compromised (Queiroz et al., 2006).
Pesticides: Some organochlorides may cause damages by concealing or blocking steroid hormones that control growth and sex, especially estrogen (female sex hormone) and testosterone (male sex hormone). For the estrogen to produce its effects in the organism, in the same way as the other hormones, it is necessary to connect them to determined protein cells, called “receptors”. The fitting of the receptor and the hormone is complex and extremely precise. Estrogen is essential for the normal development of the male and female reproductive organs, during fetal life, both in human beings and animals. For this reason, it is not surprising that organochlorides that conceal and block estrogen may indeed cause devastating effects in the development of the fetus’ reproductive system. The effects on the offspring are permanent and irreversible. According to a study held in India, a group of men who worked with organochlorine pesticides, such as Dichloro-Diphenyl-Trichloroethane (DDT), presented a reduction of fertility when compared to a less exposed group. There was also a significant increase in stillbirths, neonatal mortality and congenital defects in infants born to these men. Recent studies also indicated that occupational exposure to dioxins reduces the level of male sex hormone, the testosterone. During the Vietnam War, the soldiers who used Agent Orange, contaminated with dioxins, presented reduction in size of testicles (Rupa et al., 1991; Wole et al., 1995).
Lead: The effects of lead poisoning range from clear and clinical to subtle and biochemical. They involve several systems of organs. In adults with excessive or even incidental occupational exposure, the concern is peripheral neuropathy and chronic nephropathy. Not to mention the gastrointestinal and reproductive systems which are also targets of lead intoxication. There is evidence that heavy exposure to the inorganic lead alloy is harmful to the quality of semen. Studies on the quality of human semen suggest that the adverse effects of lead would be low sperm concentration and reduced motility, in people with chronic exposure of Pb-S at level 40-50 µg.dL-1 (ATSDR, 1999). Bonde et al. in 2002 concluded that the adverse effects of lead on testicular function in concentrations below 45 µg.dL-1 are improbable. Lead is only found in the cytoplasm of macrophages in the interstitial tissue, but it is able to cross the hemato-epididymal barrier (Marchlewicz, 1994).
Mercury: It has been considered an environmental pollutant of the highest risk to human health; therefore, the one studied the most. The biological effects of this metal and its derivates are extremely varied, comprising from cytological and reproductive effects (mainly teratogens) to neurological ones, the latter being well established. According to few studies referring to male fertility, it was possible to see that fertility was not affected by an average level of mercury around 50µg/l. However, significant loss of libido after long periods of exposure to mercury (level 44 000 µg/m3 in the air) was also observed. The appearance of abortions and congenital malformations after long periods of exposure to mercury by fathers is controversial (Alcser et al., 1989; WHO, 1991).
Cadmium: The exposure to cadmium affects more than 1 million workers a year in the United States, in the period of 10 to 30 years in the human being. Cadmium may cause direct injury in the testicles by vascular alteration. According to World Health Organization (WHO, 1991), the high level of exposure to cadmium occurs when, through a blood test, numbers over 10 µg/L can be observed. Its effect is evident in Sertoli cells, showing alteration in its morphology, degeneration of its seminiferous tubules, testicular atrophy and, in some advanced cases, deficiency in the production of androgenic hormones and necrosis of tissue. Cadmium may also interfere in the mitochondrial enzymes (Telisman et al., 2000; Kidambi et al., 2003).
Copper: It may compromise male infertility, since it is able to alter the normal spermatogenesis due to the action of follicle-stimulating hormone in the receptors (Queiroz et al., 2006).
Both authors share a leadership in a CNPq research group certificated by PUC/MG. They worked together in designing this research. The first author produced the database. The study is part of the pos-doctor from the first author. The analysis and the interpretation of data, the drafting and the revision were a product of discussion between them.
MATERIAL AND METHODS
The data for the present study were obtained from the authors` database regarding 24.280 infertile men in the period of February/1992 to February/2003 evaluated in the city of Belo Horizonte - MG - Brazil - in clinics of gynecology, human reproduction and centers of general practice. These individuals belonged to a range of infertile couples (couples without children after two years of coitus planning to have children) and apparently the woman was healthy in this context.
The infertility period varied from 2,1 to 16,4 years, with the mean period of 6,7 years. All the individuals included in the present study were born and live in the referred cities or were born in other cities but have now been living in the referred city for at least 20 years. After the geographic distribution of these individuals, 219 cities in the state of Minas Gerais presented cases. The age in these individuals ranged from 21 to 50, with the mean age of 37, 2, divided into three groups: the first between 21 and 30 representing 27% of the group; the second between 31 and 40 with 45% and the third between 41 and 50 with 27, 9%.
To determine the diagnosis of male infertility, the data found were supported by clinical and complementary examination for each case, according to WHO. The individuals evaluated were submitted to thorough medical anamnesis, hormonal dosages of FSH, LH, free and total testosterone and at least two semen analyses with the interval not inferior to 15 days between one and the other. Complementary examinations with the attempt to enhance the diagnosis were added in some cases, such as ultrasonography, CAT scan, G-banded karyotype, highresolution karyotype, genetic study of Y-chromosome micro deletions, genetic study of cystic fibrosis, testicular biopsy, specific serology, etc.
In the sequence, the incidence of the etiologies found was compared to the data from WHO, through the works of Comhaire et al. ,1987. Means and standard deviations were assessed with the use of Matlab® statistics program. The Student’s t-test was used with the level of significance of 0,05.
The present research was submitted to the Ethics and Research Committee of PUC Minas according to the requirements of Res. CNS 196/96 and its complements, being totally approved, without exceptions, in detailed report dated December 09/2003.
RESULTS
In the present study, 102 individuals (0, 42%) were estimated for this set of causes (Table 1). These data did not present significant difference in relation to the data from WHO (Irvine, 1998), that is, 0,3% (p>0, 05). This classification was characterized in 27 municipal districts, distinguishing Belo Horizonte with 39 cases. The district of Contagem accounted for 11 cases, Uberaba 06 cases, Juiz de Fora, Uberlândia, Ouro Branco and Betim 05 cases each, Pará de Minas, Diamantina and Curvelo 03 cases each. In 17 municipal districts, 01 case was catalogued in each one of them.
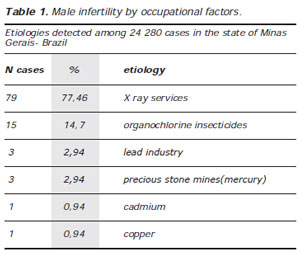
Table 1. Male infertility by occupational factors.
The professionals that work in X: ray services, totaling 79 individuals (77, 46%), were the most relevant finding among the causes of male infertility by occupational factors. In 15 individuals (14, 7%), the cause of infertility was due to exposure to organochlorine insecticides such as DDT and its prototype. These people were rural producers who alleged having worked with these substances for at least 10 years, under daily exposure, since the insecticides were applied in the plantations. Three cases of infertility (2, 94%) were reported in workers in the lead industry. The same number of cases (three) and the same incidence (2, 94%) were found in workers in precious stones mining, due to their exposure to mercury. The exposure to cadmium and copper was able to generate male infertility in one individual each (0, 98%).
DISCUSSION
The manifestations of occupational tendencies in the male reproductive function have called the attention of several researchers. By exploring regional differences, it is possible to increase the value of genetic and environmental impacts and lifestyle in man. The 21st Annual Meeting of the European Society of Human Reproduction and Embryology (ESHRE), held in Copenhagen - Denmark in June / 2005, concluded by observing the tendency of an increase in the number of men who need treatment in the reproductive sphere of up to 7% in the next decade.
This concern was always object of study in several European countries. Making an analysis, for instance, of the level of fertility in several European countries, greater sperm concentrations were found in Finnish people as compared with Scottish and Parisian people. These studies deserve prestige in the scientific field for the amplitude of the number of individuals studied and for the sampling diversity. This difference was also found when the comparison was made among young men (Jorgensen et al., 2002).
Specifically in relation to the Scandinavian countries, where studies in epidemiology of male infertility are advanced, recent studies have shown that the difference between Denmark and Finland, regarding waiting time to achieve pregnancy, is related to the high rates of seminal quality in Finnish men as compared with a corresponding group of Danish men. It is interesting to observe that the population of Finland is genetically similar to the population of Denmark. However, the variations in seminal quality reach 30% favoring Finland (Jensen et al., 2001).
Interesting reports show the variations in different regions in France (Auger et al., 1995; Bujan et al., 1996), where there is a periodical publication of the ranking of etiologies of male infertility and the number of children born through human reproduction techniques in the French specialized centers.
In the United States, Fisch et al. in 1996 reported a lower rate of sperm concentration in men born in Columbia than in New York, Minneapolis, Minnesota and Los Angeles, ranging from 59 x 106/mL to 103 x 106/mL. The establishment of universal criteria in fertility is objective of questionings. The variability is also observed in our country. Some researchers have valued the need of establishing regional criteria for the definition of normality parameters of semen in Brazil (Marinelli et al., 2003).
In the present study, the city of Belo Horizonte was responsible for 49, 4% of the findings in male infertility as a result of ionizing radiations (100% of workers in radiology clinics). The city of Uberaba showed the greatest incidence (33, 4%) of infertility cases caused by organic chlorides (DDT). Most of these individuals were workers in the rural area who constantly used these substances in their daily work on the land. The three cases of infertility by lead, due to occupational factors, were registered in Ipatinga, Caeté and Nova Lima, cities traditionally working with metal in the state of Minas Gerais.
The city of Diamantina was the focus of all three cases of infestation by mercury. The city is one of the main diamond minings in the state and mercury is used to facilitate the separation and cleaning of the material obtained in the plow in the small rivers. The metals cadmium (in the city of Ouro Branco) and copper (Uberlândia) presented 01 case each in the findings of male infertility by occupational factors.
Although traditional parameters of seminal quality can be easily measured., a significant change in the seminal profile may not be an absolute sign of a lesion in the male reproductive tract. A change in the seminal quality does not necessarily have to lead to clinical abnormalities. The reduction of male fertility can be evidence of systemic disease but it would be better having evaluation methods of male infertility by occupational factors (Levine, 1983). Many types of exposures and chemical products were shown to affect the quantity and quality of the human semen. In the literature, there are reviews that focus on occupational effects at the intratesticular level, such as the effects of dibromochloropropane. Prolonged heat is clearly harmful to spermatogenesis. The studies on occupational heat, radiation and chemical exposures and their effects on the semen were revised. Therefore, there are reasons to suggest that human seminal parameters can be used as valuable indicators of toxicity by the human body and, in the future, be able to better explain these effects due to occupational and environmental factors (Lahdetie, 1995).
Some studies tried to determine the association between exposure to occupational factors and male infertility. For this, a retrospective case control study was made using the data collected between 1991 and 1997 in nine American clinics. It was possible to observe an association between infertility and occupational factors such as exposure to radiation. There was no significant association in individuals exposed to electromagnetic cables, solvents, some pesticides and stress at work (Gracia et al., 2005). It is important to emphasize the difficulty in evaluating, in numbers, the incidence of infertility in one population since the prevailing estimate is usually computed in couples that come for appointments. Therefore, there are a significant number of men who present fertility problems and do not search for evaluation for their cases. The number of infertile men who seek help in a doctor is increasing every decade, probably because of the fall of some taboos and, without a doubt, because of the almost generalized explanation showing the difference between the concepts of sexual power and fertility.
It is very important for the couple to come to interviews and examinations not only for mutual support but also for the understanding of what is happening in relation to the investigation and choice of treatment. This involvement is fundamental for the couple’s motivation and basic when establishing trust in the professional, based on a systematic in clinical approach and in safety , in choosing a determined therapeutical conduct.
The expressive sampling of etiologies in male infertility by occupational factors among men in this study (102) and the number of municipal districts where the data were collected (27 districts), associated to the clinical conditions, qualify these etiologies as predictiveevolutionary markers of reproductive health in the state of Minas Gerais, similar to what takes place with populations in other parts of the world.
This population-based study has the objective of generating information to be practiced in the production and implementation of health programs as well as prevention programs.
Irvine DS. Epidemiology and aetiology of male infertility. Hum Reprod 1998; 13 (Suppl 1): 33-44.
Robaire B, Pryor JL, Transler JM. Handbook of Andrology. Lawrence: Allen Press; 1995.
Sheiner EK, Sheiner E, Hammel RD, Potashnik G, Carel R Ind Health 2003;41: 55-62.