JBRA Assist. Reprod. 2011;15(1):15-18
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2011.15.1.02
Embryo viability after revitrification with Vitri-ingá® method
Viabilidade embrionária pós re-vitrificação pelo método Vitri-ingá
1Universidade do Vale do Itajaí (UNIVALE), Animal Reproduction Department, Rua Uruguai, 458 - Centro, Caixa Postal 360, 88302-202, Itajaí, SC - Brazil
2Universidade Federal de São Paulo (UNIFESP), Human Reproduction Department, Rua Botucatu, 740, 04023-900, São Paulo, SP - Brazil
3Universidade Estadual de Maringá (UEM), Avenida Colombo, 5790, 87030-121, Maringá, PR - Brazil
4Materbaby - Reprodução Humana, Avenida XV de Novembro, 1232, 87013-230 - Maringá, PR - Brazil
Objetivo: A proposta deste estudo foi avaliar os efeitos da revitrificação no desenvolvimento de embriões de camundongo através do método Vitri-ingá®.
Materiais e Métodos: Estudo animal randomizado e in vitro foi realizado com fêmeas híbridas (Balb C x C57 Bl/6). Um total de 253 embriões de 2 células foram selecionados e divididos em 3 grupos: G1 embriões frescos, G2 embriões vitrificados e G3 embriões revitrificados. Após o aquecimento os embriões foram cultivados em meio Global® até completarem seu desenvolvimento. Foram comparadas as taxas de blastocisto e eclosão.
Resultados: Blastocistos obtidos nos grupos G1 (99,3%) e G2 (88,0%) não foram significativamente diferentes, mas foram significantemente maiores quando comparadas ao meio G3. Não houve diferença significativa nas taxas de eclosão entre os grupos G2 e G3, mas elas foram significantemente menores que a do grupo controle.
Conclusão: Apesar do dano cumulativo causado por 2 processos sucessivos de vitrificação, os resultados sugerem que o protocolo de revitrificação de embriões com o método Vitri-ingá® tem potencial para ser rotineiramente usado em laboratórios de reprodução assisitda.
Key Words: vitrificação, embrião, camundongo, blastocisto, eclosão.
ABSTRACT
Objective: The purpose of this study was to assess the effects of revitrification on the development of mice embryos using the Vitri-ingá® method.
Methods: Randomized in vitro animal study was performed with Hybrid Balb C x C57 Bl/6 female mice. A total of 253 two-cell embryos were selected and randomly assigned to three groups: G1 fresh embryos; G2 vitrified embryos; and G3 revitrified embryos. After warming, vitrified and revitrified as well as fresh embryos were cultivated in Global® medium until its complete development. Blastocyst and hatching rates were analyzed and compared.
Results: Blastocyst rates obtained in groups G1 (99.3%) and G2 (88.0%) were not statistically different, but were both significantly higher when compared to group G3. There were no significant differences in the hatching rates between the groups G2 and G3, but they were both significantly lower than group G1.
Conclusion: Despite the cumulative damage caused by two successive vitrification processes, the results found suggest that the embryo revitrification protocol with the Vitri-ingá® method has the potential to be routinely used in assisted human reproduction laboratories. .
Key Words: Revitrification, embryo, mice, blastocyst, hatching.
INTRODUCTION
Since the first successful in vitro fertilization (IVF) in humans in 1978, reproductive medicine has rapidly progressed with high rates of success being reported. This important medical advance has led to the necessity to give an appropriate destination to excess embryos. As a result, supranumerary blastocysts are normally cryopreserved in IVF-ET cases, either by slow-freezing methods (Menezo, 1992; Gardner 2003) or vitrification (Reed, 2002), which has permitted the transfer of a reduced number of embryos per cycle, avoiding multiple pregnancies and providing the opportunity for more than one transference attempt after just one stimulation cycle (Anderson, 2005). Cryopreservation has also been useful in cases of unexpected sudden cycle cancelling, either due to psychological disturbances of the patient (Özmen, 2006), and the incorrect administration of the prescribed medication (Oakes, 2008). In those special circumstances, when embryos had been cryopreserved and thawed previously, the need of a new cryopreservation procedure emerges.
Recent studies have demonstrated that cryopreservation using different vitrification methods presents better survival (Loutradi , 2008), blastocyst formation, implantation and gestation rates in humans (Balaban, 2008), when compared to the slow-freezing protocol. Vitrification is characterized by the ultra high cooling rates (>10.000 ºC/min), in which embryos are immediately immersed into liquid nitrogen either in open or closed systems, after the quick exposition to high concentration of cryoprotectants (Rall &, Fahy , 1985; Vajta & Kuwayama, 2006). During this contact, embryos go through rapid cellular dehydration leading to the immediate solidification of the solution due to the high increase of viscosity during cooling (vitrification), avoiding the formation of intracellular ice crystals (Fahy, 1984; Liebermann, 2002). As a result, vitrification of embryos, as well as of oocytes, has recently been widely used in assisted reproduction centers (Selman, 2009).
The revitrification of embryos becomes, therefore, a potentially useful technique in assisted human reproduction centers in special circumstances. However, before suitable human embryo revitrification protocols may be established, animal studies must be carried out in order to assess the safety and the efficacy of this technique. Hence, the objective of this study was to analyze the revitrification of mice embryos using a new vitrification method (Vitri-ingá®).
MATERIALS AND METHODS
]Superovulation and embryo collection
Embryos were obtained from 15 hybrid C57 Bl/6 x Balb C female mice 4 to 5 weeks old, which were superovulated with the intraperitoneal administration of 10 IU of eCG (Equine Chorionic Gonadotrophin - Novormon® - Synthex, Buenos Aires, Argentina), followed by 10 IU of hCG (Human Chorionic Gonadotrophin - Vetecor® - Calier, Barcelona, Espanha) 48 hours later. Following the hCG injection, female donors were paired with males of the same strain overnight. In the next morning females were removed from males and checked for the presence of vaginal plug. Fourty-four hours later, females were sacrificed by cervical dislocation, and two-cell embryos were collected from the uterine tubes with HTF-Hepes medium (Life Global, USA) + 10% of bovine fetal serum (BFS - Gibco, New York, USA) (Bertolini, 2005). A total of 253 two-cell embryos were morphologically assessed and selected according to number, as well as the degree of fragmentation and uniformity of blastomeres, as described elsewhere (Roberston & Nelson, 1998), and randomly allocated to the experimental groups.
VITRI-INGÁ® METHOD
Both the vitrification and revitrification of embryos in this study followed the protocol established by the Vitriingá® method, described below (Fachini, 2008). All the equipment and materials used for the vitrification/thawing procedures were supplied by Ingámed Ltda. (Perobal, PR, Brazil) and consisted of: the Vitri-Equip, an expanded polystyrene box (44.0 x 19.5 x 15.0 cm) containing 2 stainless-steel containers of different sizes for liquid nitrogen; one container measuring 18.5 x 6.0 x 8.8 cm, in which there is a small stainless-steel rack for cooling straws, and another one measuring 5.3 x 5.3 x 10.0 cm for vitrification (Figure 1); the vitrification solutions VI-1 and VI-2; the warming solutions DV1, DV2, and DV3; the vitrification strip, an apparatus consisted of a fine, very thin polypropylene film (0.7 mm thick) with a specially designed round tip, in which there is a minute hole to receive the embryo, connected to a hard and thicker plastic handle (Figure 2); and the protective plastic sheaths. Definition of groups
G1 (Control): After collection, embryos (n = 87) were immediately placed into microdrops (10 embryos/drop) of 30µL of Global medium (LifeGlobal®, USA) supplemented with 10% BFS and cultivated for 120 hours.
G2 (Vitrified): Immediately after collection, embryos (n = 82) were initially placed into 200 µL of VI-1 solution and equilibrated for 8 to 15 minutes. After that, groups with three embryos each were immersed into three consecutive 20 µL drops of VI-2 solution, remaining for 20 seconds in each one, and immediately placed into the hole of the vitrification strips. Excess medium was aspirated and the strips were directly immersed into liquid nitrogen. The total time from the moment embryos were placed into the vitrification solution until its immersion into liquid nitrogen was between 50 to 60 seconds. The plastic sheaths, which had been previously cooled for at least two minutes in liquid nitrogen vapour on the metal rack inside in the Vitri-Equip, were vertically immersed into liquid nitrogen. The Vitri-Ingá strips with the vitrified embryos was then individually inserted into the plastic sheaths for safe storage, and transferred to a liquid nitrogen tank.

Figure 1. Vitri-Equip: Expanded polypropylene box with 2 stainless steel containers for cooling and vitrification
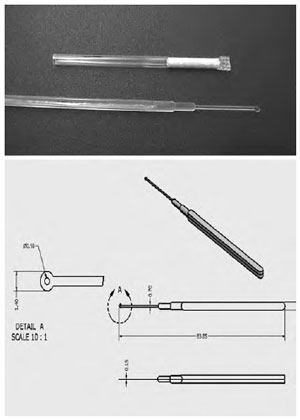
Figure 2. Vitri-Ingá vitrification strip and protective sheath
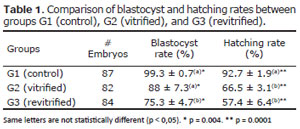
Table 1. Comparison of blastocyst and hatching rates between groups G1 (control), G2 (vitrified), and G3 (revitrified).
Embryos remained cryopreserved for at least 24 hours. During warming, the strips were removed from the protective sheaths and immediately plunged into DV-I warming solution for 1 minute at 37ºC. Recovered embryos were transferred to 100µL of DV-II solution for 3 minutes at room temperature and finally kept for 5 minutes in each one of the 2 drops containing 100µL of DV-III solution for rinsing (Vajta & Nagy, 2006). Warmed embryos were placed into culture following the same protocol used by group G1. All vitrification / warming procedures were carried out in room temperature.
G3 (Revitrified): Embryos (n = 84) were vitrified and warmed as for group G2, and cultivated for 24 hours as for G1. Embryos that presented cleavage were revitrified, as described above, and at least 24 hours later rewarmed and placed into culture for another 96 hours.
Assessment criteria and statistics
Post-vitrification viability, blastocyst and hatching rates were analyzed using Anova followed Tukey’s test. Results with p < 0.05 were considered significant. Embryos were considered viable when after rehydration presented ≥ 50% of whole blastocysts and intact zona pellucida. Blastocyst rates were recorded for embryos that initiated the cavitation process, and hatching rates in the presence of zona pellucida rupture.
RESULTS
Blastocyst and hatching hates obtained in this study are presented in table 1. Group G1 (control) presented blastocyst and hatching rates of 99.3 ± 0.7% and 92.7 ± 1.9%, respectively. In group G2 (vitrified), 98% of embryos survived the vitrification process, among which 88 ± 7.3 % reached blastocyst stage and 66.5 ± 3.1% hatched. In Group G3 (revitrified), 95% and 81% of embryos survived the first and the second vitrification processes, respectively. Blastocyst and hatching rates after revitrification were (75.3%) and (57.4%), respectively.
There were no statistically significant differences in the blastocyst rates between groups G1 and G2. However, embryos in group G3 presented blastocyst rates significantly lower to the other groups (p = 0.004). Embryos in group G1 presented an excellent hatching rate (99.3%) after 5 days in culture, which was significantly higher when compared to groups G1 and G2 (p = 0.0001), with no significant differences being observed between G2 and G3.
DISCUSSION
The current study assesses the effects of revitrification on murine embryos using the Vitri-ingá® method by comparing blastocyst and hatching rates to those of fresh (control) and vitrified murine embryos. This study shows the potential of revitrification as a routine procedure in assisted human reproduction centres. Our objective in this study was to obtain reliable data concerning the embryo survival after going trough the vitrification process twice. For this reason we have opted for the first vitrification process with cleavaged embryos in two-blastomere stage. After warming, embryos were kept in culture for 24 hours until evolving to four to eight-cell stage, after which re-vitrification was carried out. After the second warming, embryo viability was evidenced by embryo development up to blastocyst stage.
Vitri-ingá® is a novel vitrification method similar to the Cryotop method (Kuwayama, 2005). The main difference between these methods is the minute hole at the tip of Vitri-ingá’s thin plastic stem in which embryos are lodged during vitrification. This method facilitates the removal of excessive cryopreservation solution by aspiration, leaving just 0.1 μl around the embryo and permitting cooling rates of 22,800 ºC/min (Kuwayama, 2005). The Vitri-ingá method was initially tested in an animal study, which presented a survival rate of 86% after vitrification/thawing of bovine oocytes matured in vitro (Almo- din, 2008). Additionally in another study, this time using human oocytes, the Vitri-Ingá method again demonstrated good results with survival, fertilization and pregnancy rates of 80.5%, 76.6% and 24.5%, respectively (Fachini, 2008). One of the possible criticisms of the vitrification technique using Vitri-Ingá is the fact that it is an open system, i.e., the oocyte is placed into direct contact with liquid nitrogen during vitrification. This raises the issue concerning the theoretical possibility of contamination by liquid nitrogen. Although the risk of contamination by liquid nitrogen contact must be taken into consideration, no documented cases of diseases transmitted due to the transference of vitrified embryos have been reported. The development of a technique using a hermetically sealed vitrification device could eliminate the potential risks of contamination.
The need for doubly crypreserving embryos has emerged out of punctual needs in human reproduction centers such as psychiatric problems that occurred during the second attempt after cryopreserved embryos had already been thawed (Özmen, 2006), incorrect administration of prescribed drugs (Oakes, 2008), or blastocysts that were unduly thawed because of a clinical error (Son, 2005). Due to ethical and legal reasons, warmed embryos must have an adequate destination and a new cryopreservation procedure becomes necessary.
There are several reports in the literature of successful pregnancies obtained with human embryos that were cryopreserved twice. In recent a study using the slowfreezing method, the authors reported a gestation rate of 35% in a group of 14 patients when embryos in the 2 pronucleus (2PN) stage were doubly cryopreserved (Sills, 2009). In another recent study, 27 human embryos originated from 15 assisted fertilization cycles were revitrified in the 4 to 8 cells stage, with 96% of blastocysts surviving the procedure and being transferred to patients, with an implantation rate of 35%, and gestation confirmed in 47% of cases (Hiraoka, 2007). Despite this success, these have been mostly case reports, following no previously defined methodologies, which make a comparative analysis difficult.
Animal reports show that blastocyst rate for mice embryos vitrified in the two-cell stage vary, between 52 and 90%, with no significant differences when compared to controls (Graves-Herring & Boone, 2009; Uechi 1999; Miyake , 1993; Mello, 2001), which is in accordance with the present study. The hatching rate drop for vitrified embryos is always observed but it does not seem to be related either to the protocol, as it also occurs with slow-freezing protocol, nor with the different cryoprotectants used (Sheehan, 2006; Ramezani, 2005). Possibly, this decrease may be linked to the stress that the embryo is submitted to after the exposition to low temperatures, the hardening of the zona pellucida, or even the toxicity of cryoprotectants.
Although studies carried out in murine (Ramezani, 2005) and bovine (Gómez, 2009) embryos report that vitrification and revitrification result in lower numbers of cells in the blastocyst, authors believe that this decrease does not negatively influence embryo development (Vitale, 1997). Lower hatching rates for murine embryos vitrified consecutive times have been associated to zona pellucida hardening, as the number of cells in the blastocysts was not different from non-vitrified embryos (Ramezani, 2005). Possibly, the reduction in the number of cells and zona pellucida hardening may have contributed to the lower hatching rates observed in this study.
Despite the observed cumulative damage caused by the two vitrification processes, blastocyst and hatching rates of 75% and 57% were obtained in this in vitro murine study. These results suggest that the embryo revitrification protocol with the Vitri-ingá® method has the potential to be used in assisted human reproduction laboratories when the circumstances may demand it. Nonetheless, in order that this technique may be used with greater efficiency and safety, further assessments investigating the damages caused on the embryo by the first and the second vitrification process must be performed.
ACKNOWLEDGEMENT
The Vitri-Ingá® equipment used in this study was provided to Universidade do Vale do Itajai (Univale) without charge by Ingamed Ltda (Perobal - Pr-Brazil)
Vajta G, Kuwayama M. Improving cryopreservation systems. Theriogenology 2006;65:236-44.