JBRA Assist. Reprod. 2011;15(02):19-30
ORIGINAL ARTICLE
doi: 10.5935/1518-0557.2011.15.2.03
Twenty years of Assisted Reproductive Technology (ART) in Latin America.
Assisted Reproductive Technology in Latin America.
ABSTRACT
Introduction: Since 1990, the Latin American Registry of Assisted Reproduction (RLA) has registered ART procedures performed in Latin America. The RLA has increased its regional coverage including to date more than 80% of ART cycles performed. 140 centers enter their data directly on line, and an administrative office collects and analyses the data.
Material and methods: This paper analyses trends over the last twenty years, as well as biomedical data corresponding to ART procedures initiated between 1990 and 2009, and babies born up to 2010. Overall, the data include 275,883 embryo transfer-cycles, 71,875 deliveries and the birth of 95,436 babies.
Results: Some of the major changes include: an increase in the age of female partners undergoing fresh, autologous embryo transfers; and a marked shift towards the use of ICSI over IVF. As expected, there has been a steady increase over the last ten years in the delivery rates with at least one live born per embryo transfer, reaching 25.3% in IVF/ ICSI cycles, and 31.6% in OD cycles. Over the years, there has been a progressive but slight decrease in the mean number of ET, but still, almost one third of all births are either twins or triplets. In the last 15 years, the proportion of transfers of one or two embryos has increased from 11 and 17% in 1995, to 14%· and 43% respectively in 2009,
Conclusions: Access to ART has experienced a meager increase during the period covered in this report.Our region faces two main challenges: to facilitate access to ART and to decrease the rate of multiple births.
Key words: ART registry Latin America
RESUMO
Introdução: Desde 1990, o Registro Latinoamericano de Reprodução Assistida (RLA) tem registrado os procedimentos de Reprodução Assistida (RA) realizados na América Latina. O RLA aumentou sua cobertura regional, incluindo dados de mais de 80% dos ciclos de reprodução realizados. Hoje 140 centros inserem seus dados diretamente on line, e uma central administrativa coleta e analisa os dados.
Material e métodos: Este artigo analisa as tendências dos últimos 20 anos, bem como dados biomédicos correspondentes aos procedimentos de RA iniciados entre 1990 e 2009, e recém-nascidos até 2010. Globalmente, os dados incluem 275.883 ciclos com transferência de embriões, 71.875 partos e o nascimento de 95.436 bebês.
Resultados: Algumas das principais mudanças incluem: aumento da idade das parceiros do sexo feminino submetidas a transferência de embriões à fresco, não-doados, e uma mudança acentuada para a utilização da ICSI. Como esperado, houve um aumento constante ao longo dos últimos dez anos nas taxas de partos, com pelo menos um nascido vivo, por transferência de embriões, atingindo 25,3% em ciclos de FIV / ICSI e de 31,6% em ciclos de OD (Ovo-Doação). Ao longo dos anos, tem havido uma diminuição progressiva, leve, do número médio de embriões transferidos (ET), mas ainda assim, quase um terço de todos os nascimentos são de gêmeos ou trigêmeos. Nos últimos 15 anos, a proporção de transferências de um ou dois embriões aumentou de 11% e 17% em 1995, para 14% e 43% em 2009, respectivamente.
Conclusões: O acesso a RA teve um aumento insuficiente durante o período abrangido por este relatório. Nossa região enfrenta dois desafios principais: facilitar o acesso à RA e diminuir as taxas de nascimentos múltiplos.
Palavras chave׃Reprodução assistida, Registro, América Latina
RESUMEN
Introducción: Desde el año 1990, el Registro Latino Americano de Reproducción Asistida (RLA) ha registrado y publicado los procedimientos de reproducción asistida realizados en la región. El RLA ha incrementado su cobertura de manera continua, incluyendo a la fecha más del 80% de los ciclos de reproducción asistida realizados en la región. En la actualidad, 140 centros ingresan voluntariamente su información en un programa en línea, y una oficina administrativa central recopila y analiza esta información de manera periódica.
Material y métodos: El presente trabajo analiza las tendencias en los procedimientos de reproducción asistida realizados en los últimos veinte años, y la información biomédica de los procedimientos iniciados entre 1990 y 2009, así como los bebés nacidos hasta septiembre del 2010.
Resultados: En total se analizan 275,883 transferencias embrionarias; 71,875 partos y las características de 95,436 bebés. Algunos de los principales tendencias observadas en este periodo incluyen: aumento en la edad de las mujeres sometidas a la transferencia de embriones autólogos; una marcada preferencia por el uso del ICSI por sobre la FIV; una mejoría sostenida en la tasa de parto con al menos un recién nacido vivo por transferencia embrionaria, que llegó a 25.3% en ciclos de FIV/ ICSI y 31.6% en ciclos de OD. Asimismo, en este período ha disminuido en forma sostenida, pero en poca cuantía, la media de embriones transferidos; a pesar de eso, casi un tercio de todos los partos son dobles o triples. La proporción de transferencias embrionarias de uno y dos embriones ha aumentado de 11 y 17% en 1995 a un 14 y 43% en 2009, respectivamente.
Conclusión: El acceso a técnicas de reproducción asistida ha experimentado un aumento mínimo. Nuestra región se enfrenta a dos grandes desafíos: aumentar el acceso a las técnicas de reproducción asistida y disminuir la frecuencia de partos múltiples.
Palabras claves: Reproducción Asistida en latino América
ACKNOWLEDGEMENTS
The authors wish to acknowledge the work by Veronica Galdames, BSc. Her commitment to the administration and continuous improvement of the Latin American Registry has been fundamental in achieving the recognition gained over these twenty years. We also wish to thank the voluntary contribution of today’s 140 centers reporting to the Latin American registry of assisted reproduction (see under Participating Institutions).
INTRODUCTION
The first birth of an IVF baby was reported in Latin America in 1984. During the next five to six years the use of this technology expanded rapidly in Argentina, Brazil, Mexico, Colombia and Chile. Little is known about the number of attempts and the number of babies born until 1990 when the Latin American Registry of Assisted Reproduction (RLA) was established. This initiative was the first multinational / regional registry which had mainly five objectives:
1- Collect and disseminate the information on ART procedures performed in the region.Nineteen IVF centers from 12 countries initiated this registry. Twenty years later the registry has expanded and a vast proportion of centers performing ART report to RLA every year. The RLA is a voluntary activity, which collects and publishes summary of regional data on a yearly basis. The first step was to develop standardized forms and distribute them among participating centers. During the nineties, the forms for data collection were adapted from those developed by the international working group for registers on assisted reproduction, today, International Committee Monitoring Assisted Reproductive Technology (ICMART). Throughout the years, these have been further developed according to regional interests and the uninterrupted advancement of science and technology.
2- Assess and monitor different type of interventions and their outcome.
3- Monitor trends on safety and efficacy among centers, countries and regions.
4- Empower infertile couples in their capacity to evaluate risks and benefits when exposed to ART procedures.
5- Develop a robust database for epidemiological studies.
In 1990, nineteen centers reported a total of 2,415 initiated cycles; and in spite of the fact that increasing number of centers were becoming part of this activity, in its fourth year, the coverage of the registry was suboptimal and there were concerns about the reliability of the information provided by certain institutions. To address these issues, in 1996, representatives from each of the 59 centers reporting to the RLA founded the Latin American Network of Assisted Reproduction (REDLARA). Latin America was divided into five sub-regions and a regional director was appointed for each one. Human and economic resources were allocated to start a regional educational program focused on preparing embryologists and clinicians for the process of center accreditation, which started on the following year.
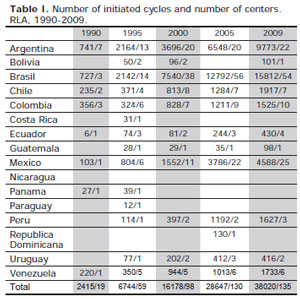
Table I. Number of initiated cycles and number of centers. RLA, 1990-2009.
Since 1996, all centers willing to become members of REDLARA undergo a periodic accreditation process whereby infrastructure, equipment, personnel, use of appropriate consent forms, and veracity of the information reported to the RLA are checked for quality and consistency.
After 20 years, the number of participating centers has increased from 19 to 140, reaching 38,020 initiated cycles per year, which represents more than 80% of ART cycles performed in the region. Today, Brazil contributes with 41.6% of the initiated cycles, Argentina, 25.7% and Mexico with 12.1%; while the remaining cycles are from Colombia, Chile, Uruguay, Venezuela, Peru, Ecuador, Guatemala, and Bolivia (Fig 1).
This communication includes the outcome of ART procedures initiated between January 1990 and December 2009. It also includes the outcome of babies born up to September 2010.
DATA COLLECTION, ANALYSIS AND COMMUNICATION
Initially, data was compiled using printed forms, sent by mail or fax. In 1990 special software was developed for electronic collection of data. Although it had a builtin system to check for inconsistencies, it still required excessive interaction between the administrative office and each individual centre. Today, participating institutions enter their data directly online (www.redlara.com). The administrative office in Santiago, Chile, periodically extracts and analyses the data for consistency. Once all the information is cleared, and the center is checked as accredited by the RED, the data is included and published as part of RLA’s yearly report.
The terminology used in the registry is that contained in the “ICMART/WHO glossary of ART terminology” (Zegers-Hochschild et al., 2009a) (Zegers-Hochschild et al., 2009b), further translated and published in Portuguese and Spanish (Zegers-Hochschild et al., 2009a) in compliance with regulations by the World health Organization (WHO).
Along with every report, each individual center can access an electronic file prepared by RLA, containing their own data as well as their corresponding national data. As a result of the RLA initiative, today, every participating country in Latin America has a national ART database with information analyzed, verified and summarized by RLA. After approval of the participating centers, national data is also sent to the International Committee Monitoring ART (ICMART) for inclusion in the publication of the world report (International Committee for Monitoring Assisted Reproductive Technology; De Mounzon et al., 2009).
As of today, RLA keeps a complete registry of ART procedures, from 1990 up to September 2010, including in vitro fertilization (IVF), gamete intra-Fallopian transfer (GIFT), intra-cytoplasmatic sperm injection (ICSI), assisted hatching (AH), oocyte donation (OD) and the transfer of frozen/thawed embryos (FET). Overall, the data consists of 275,883 embryo transfer cycles, with 71,875 deliveries and the birth of 95,436 babies. Of these newborns, 77.2% correspond to nondonor fresh cycles (55.1% ICSI, 19.7% IVF and 2.4% GIFT and other techniques); 6% to FET cycles; and 16.8% to OD cycles.
CHARACTERISTICS OF INSTITUTIONS AND TYPE OF TREATMENTS PROVIDED IN LATIN AMERICA
From 1990 to 2009, the proportion of centers performing less than 100 cycles decreased from 63% to 24% and the largest proportion (60%) are centers providing between 100 and 500 cycles per year (Fig 2). The proportion of centers reporting ≥ 1000 cycles remains small (2-3%).
Concerning the type of treatment used, IVF and ICSI continue to represent the vast majority of treatments (71%). However, Frozen Embryo Transfer (FET) increased from 4% in 1995 to 12% in 2009. In the same interval, Oocyte Donation (OD) increased from 5 to 16%. GIFT has almost disappeared (Fig 3).
STATISTICAL ANALYSIS
Summary statistics included mean and proportions, and when appropriate, 95% confidence interval. The data presented by RLA correspond to description of observational statistics, not to the results of randomized controlled trials. Therefore the authors urge the readers to be cautious at inferring causality.
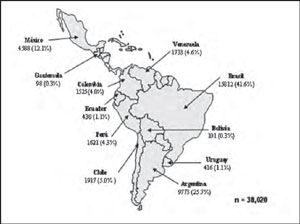
Figure 1. Number of initiated cycles by country. RLA, 2009.
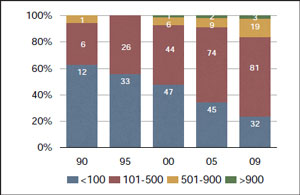
Figure 2. Distribution of centers according to the number of initiated cycles. RLA, 1990-2009.
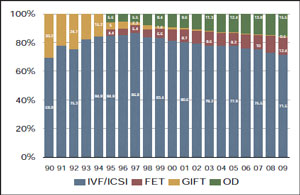
Figure 3. Proportion of different ART treatments. RLA, 1990-2009.
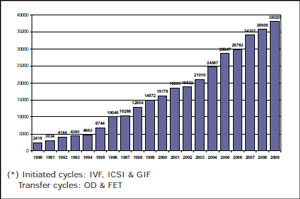
Figure 4. Number of ART cycles per year(*). RLA, 1990-2009.
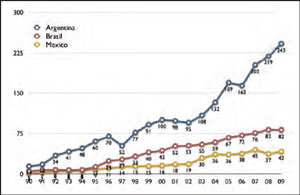
Figure 5. Access to ART procedures in Argentina, Brazil, Mexico. Initiated cycles/1,000,000 habitants.
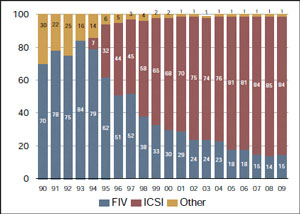
Figure 6. Fertilization technique. RLA, 1990-2009.
We used Fisher’s exact test to determine whether there was association between different categorical data. We rejected the null hypothesis, i.e. there is no association between the variables, when the p-value was <0.05.
ACCESS AND NUMBER OF ART CYCLES PER COUNTRY
Table I describes the number of initiated cycles and the number of ART centers per country from 1990 to 2009. Overall, the number of initiated cycles increased from 2,415 in 1990, to 16,178 in 2000, reaching 38,020 in 2009. Although the number of cycles more than doubled in the last ten years (Fig 4), the total number of treatment cycles per country is below the number of cycles required in each country. Overall, Latin America performs a mean of 75 cycles per million inhabitants, compared with most European countries performing between 1000 and 2000 cycles per million (Zegers-Hochschild & Nygren, 2009). Today, the country with higher access to ART treatment in Latin America is Argentina with 242 ART cycles per million, followed by Brazil with 82 per million (Fig 5).
FERTILIZATION TECHNIQUE
Since 1994 when ICSI was introduced in Latin America, there has been a continuous and preferred use of ICSI over IVF (Fig 6). ICSI represents 84% of procedures. This tendency is not related with an increment in male factor infertility, because the proportion of different diagnostic categories has remained unchanged over the past 5 years with only 30% of male factors. Although worldwide, there is an increasing tendency towards ICSI, the high proportion seen in Latin America is partly the result of some large centers that only use ICSI as a fertilization technique.
AGE OF FEMALE PARTNERS
The age of the female partner has a great impact in the outcome of any fertility treatment. Therefore, when comparing outcomes between countries or between different years, it is important to adjust the results by age. In 2000, 49% of women were ≥ 35 years and 15% were ≥ 40. In 2009 58% of treatment cycles were performed in women ≥ 35 and 18% in women ≥ 40 years. The mean age of women having autologous ART treatments have increased and therefore, the changes over the years in pregnancy and delivery rates need to consider this fact (Fig 7).
STRATEGIES FOR EMBRYO TRANSFER
Together with the age of women, the decision on the number of embryos transferred and the stage of development at the time of transfer has the highest impact in treatment outcome. It directly influences the chances of becoming pregnant as well as the rate of multiple births.
Throughout the years, there has been a steady decrease in the number of embryos transferred. Between 1995 and 2000 the number of embryos transferred decreased only slightly from a mean of 3.5 to 3.2 embryos. In the last 10 years, there has been a continuous decrease reaching a mean of 2.4 embryos in 2009. Unfortunately, the policy of number of embryos transferred does not change according to age category. Thus, the mean number of embryos transferred in women under 34 is similar to women age 35 to 39. In women above 40, the number of embryos transferred seems to be the result of embryos available rather than a policy considering safety and efficacy (Fig 8).
The proportion of 3 or more embryos transferred has decreased from 72 to 74% in the nineties to 44%, in 2009. Furthermore, the proportion of ≥ 4 embryos transferred dropped from 52% in 1995 to 10% in 2009 (Fig 9). This decrease in the number of embryos transferred is far from what has been reached by many European countries where ≥ 3 embryos are transferred in less than 8% of cases (Zegers-Hochschild et al. 2009). The highest impact in the outcome of ART in Latin America (multiple births), derives from the high proportion of ≥3 embryos transferred in women ≤ 34, which today represents 40% of transfers (Fig 10). There has been a significant drop in the proportion of 4 embryos transferred, from 40 to 60% in mid nineties to only 7% in 2009. The number of two embryo transfers has increased from 12% in 1990 to almost 51% in 2009, which is an encouraging lead towards reducing the number of embryos transferred in the region.
The proportion of elective dual embryo transfer (eDET) is slightly increasing since it was first registered in 2005. Today eDET represents 16% of all transfers (Fig 11). In women ≤ 34, where elective transferred should be extensively used, the proportion of eDET and eSET is only 19% and 1% respectively.
Concerning the stage of embryo development at the time of embryo transfer, there has been little change over the last 10 years. In 2000, when this data was first collected, 31% of embryo transfers were performed at 48 hours, 63% at 72 hours and 6% as blastocysts. In 2009, 30% of transfers were at 48 hours, 60% at 72 hours and blastocyst stage transfers increased to 10% (Fig 12).
OUTCOME OF ART CYCLES
There are different markers to measure the outcome of ART cycles. In general these are expressed as rates, with a numerator such as clinical pregnancies (CPR), deliveries (DR) and live-births (LB); and a denominator, such as initiated cycles (IC), oocyte pick-up (OPU) and embryo transfer cycles (ET). Furthermore, these can be expressed as cumulative pregnancy or delivery rate when the outcomes of frozen embryo transfers (FET) are added to the results of fresh transfers.
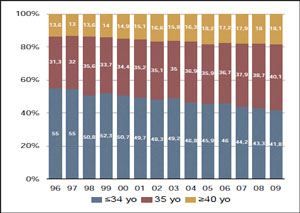
Figure 7. Percentage of embryo transfers according to age of female partner (ICSI/IVF). RLA, 1996-2009.
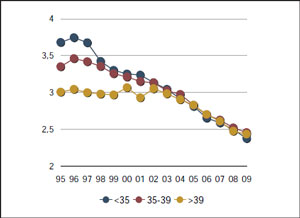
Figure 8. Mean number of embryos transferred according to age of female partner. RLA, 1995-2009.
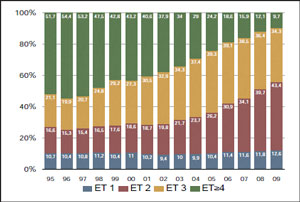
Figure 9. Distribution of transfers according to the number of embryos transferred. RLA, 1995-2009.
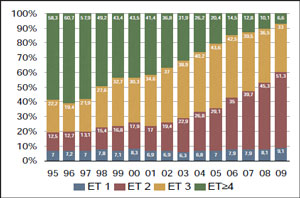
Figure 10. Distribution of transfers according to the number of embryos
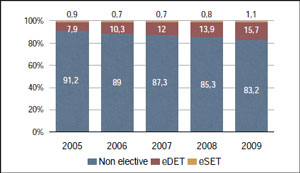
Figure 11. Proportion of eSET and eDET. RLA, 2005-2009.
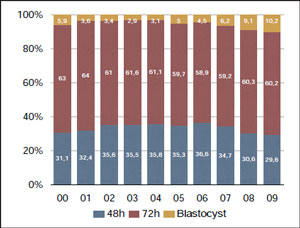
Figure 12. Embryo transfers according to stage of embryo development. RLA, 2000-2009.
A good measure of outcome should consider the well being of mother and offspring both as independent individuals and as social beings. This means, that the birth of singletons and triplets or quadruplets, although counted as one delivery constitute different outcomes, from the perspective of the babies born and their mother as well as for the family structure and society as a whole. Therefore under this concept there are big differences in single births compared with multiple births.
There is a tendency to restrict the use of “success” when a single, healthy baby is born. This has been vastly discussed and has various meanings depending on ethnic diversity, cultural variations, age of women, etc. The concept of success will not be used in this report. Markers of outcome will be restricted to CPR, DR and cumulative DR. We will also look at term and pre term birth as well as perinatal outcome (stillbirths, live births and early neonatal deaths).
AUTOLOGOUS FRESH IVF AND ICSI
The outcome of ICSI and IVF cycles are grouped together since there are no significant differences in CPR and DR with either treatment. Furthermore, as seen previously 84% of treatments performed today correspond to ICSI.
Clinical Pregnancy Rate according to woman’s age.
As expected, the CPR/ET has increased continuously throughout the past 15 years, from 31 to 42% in women < 35, with similar increments in other age categories (Fig 13). This is especially relevant considering that in the last 15 years, the mean number of embryos transferred dropped from a mean of 3.5 to 2.4 embryos. Overall, the CPR has remained very stable over the past 4 to 6 years. When comparing with other regions of the world, Latin America has a higher CPR than Europe and the Middle East, but in Latin America the number of transferred embryos is also higher (De Mouzon et al. 2009).
Clinical Pregnancy Rate according to number of embryos transferred.
It is well established that increasing the number of embryos transferred raises the chances of pregnancy. It is also well established that the quality of clinical and laboratory facilities have a strong influence in the outcome of treatment. This explains why in the past 15 years, technical improvements and the accreditation process, which determines a minimal standard of care to be part of REDLARA, have positively influenced the results of ART. Between 1995 and 2000 the CPR reached the same level when transferring 3 and 4 embryos. Furthermore, in the last ten years, the CPR when transferring 2 and 3 embryos has also leveled, reaching 37 and 39% respectively (Fig 14). The low percentage of pregnancies when transferring one embryo (17%) is mostly a reflection of cases with poor prognosis, where there were no more embryos available for transfer.
Clinical Pregnancy Rate with elective dual embryos transfer (eDET).
The possibility of selecting two embryos to transfer from a larger cohort of available embryos provides better results than those obtained when there are no more embryos available for transfer.The transfer of ≤ two embryos in a restricted group of women ≤ 34 years has increased from 19% in 1995 to 60% in 2009, while the transfer of ≥ 3 embryos decreased in half; from 80 to 40% respectively. From 1995 to 2006, there was always a clear advantage (in terms of CPR). First, the CPR with 2 and 3 embryos is very similar in this age group. Second, eDET, which is being registered only since 2005, shows an even higher CPR than the transfer of ≥ 3 embryos. In 2009 the difference of CPR of eDET and the transfer of ≥3 embryos did not reach statistical significance (p=0.330), nevertheless, this clearly shows that transferring more than two embryos does not yield better results (Fig 15). Today, a maximum of two embryos should be transferred in young women.
Clinical Pregnancy Rate according to the time of embryo transfer.
The stage of embryo development when embryos are transferred is expressed in hours after insemination, and only registered since the year 2000. Up to 2005 the time of transfer did not seem to produce great differences in outcome. However since 2006, the CPR is higher when transferring at 72 hours over 48 and the same holds for the transfer of blastocysts over a developing embryo (P< 0.001) (Fig 16).
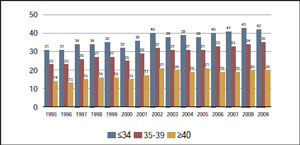
Figure 13. Clinical Pregnancy Rate per embryo transfer (CPR/ET) according to age of female partner. RLA, 1995-2009.
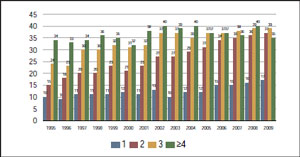
Figure 14. Clinical Pregnancy Rate According To Number of Embryos Transferred. RLA, 1995-2009.
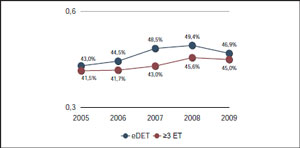
Figure 15. Comparison of Clinical pregnancy rate between eDET and ≥ 3 embryos transferred in women ≤34 years. RLA, 2005-2009.
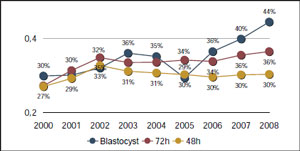
Figure 16. Clinical pregnancy rate according to stage of embryo development. RLA, 2000-2008.
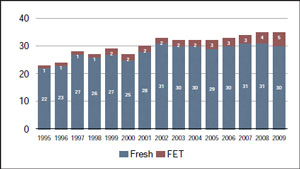
Figure 17. Cumulative Clinical Pregnancy Rate. Per 100 Oocyte Pickup cycles. RLA, 2005-2009.
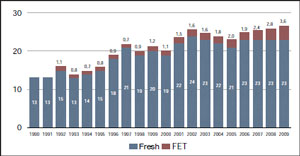
Figure 18. Cumulative Delivery Rate with ≥1 Live-born per 100 Oocyte Pick Ups. RLA, 1990-2009.
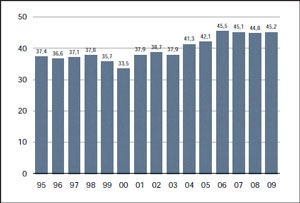
Figure 19. Clinical pregnancy per embryo transfer in Oocyte Donation (OD). RLA, 1995-2009.
Cumulative Pregnancy and Delivery Rate
Cumulative pregnancies or deliveries result from adding pregnancies or deliveries after fresh and frozen transfer, derived from one oocyte pick-up The relative contribution of FET in the overall outcome of ART can only be calculated in a cycle-by-cycle registry, and after fresh and at least one frozen/ thawed transfers have been performed. Because our registry collects summary data, this calculation cannot be performed; so we have imputed these results by adding the number of deliveries after fresh and frozen transfers in each year and divide them by the number of oocyte pick-up. As observed, the incorporation of FET to fresh autologous cycles increases pregnancy and delivery rates by an order of 4 to 5% (Fig 17 & 18).
OOCYTE DONATION (OD)
The RLA collects data corresponding to transfer cycles with OD since 1995. In the last 15 years, 32,633 transfer cycles have been registered, generating 13,743 clinical pregnancies, 10,313 deliveries and the birth of 13,878 babies.
The proportion of OD to homologous IVF/ ICSI has increased steadily, from only 8% in 1995 to 23% in 2009.
Number of embryos transferred and Clinical Pregnancy Rates.
Overall, the clinical pregnancy rate has increased from 37.4% in 1995 to a fairly stable 45% for the interval between 2006 and 2009 (Fig 19). Furthermore, the delivery rate per ET increased from 31 to 34% during the same time interval.
In these 15 years, 1,444 (4%) have been SET, 11,405 (35%) DET and 19,784 (61%) include the transfer of ≥ 3 embryos. The CPR/ET according to the number of embryos transferred (Fig 20) shows a four-fold increase in the CPR when transferring nonelected SET, from 6% in 1995 to 25% in 2009. Furthermore, until 2005, the transfer of ≥ 3 embryos yielded significantly more pregnancies than DET; however, in the last 5 years, the transfer of non elective DET yields exactly the same results (46 to 47%) as the transfer of ≥ 3 embryo; thus, the transfer of ≥ 3 embryos only contributes to multiple births.
The RLA does not register the age of the oocyte donor; it only registers the age of recipient woman at the time of ET. As reported previously (Zegers-Hochschild et al. 2010), the CPR is significantly affected by the age of the recipient. The CPR in oocyte recipients, age 35-39 years was 48% compared with 44% in women ≥ 40 (p= 0.05). Interestingly, women < 35 also have a lower CPR (45%) similar to women > 40. This could be related to a higher concentration of women with premature ovarian failure and genetic factors in this age category (Fig. 21).
FROZEN EMBRYO TRANSFER (FET)
The RLA collects data corresponding to FET cycles since 1995. In the last 15 years, 29,793 transfer cycles have been registered, generating 6,525 clinical pregnancies, 4,510 deliveries and the birth of 5,472 babies.
The frequency of FET cycles has increased over the last fifteen years. In 1995 the proportion of FET over fresh IVF/ICSI was 7%, and in 2009 it represents 18%. This increment is the result of a number of reasons, among others, an increasingly better technology yielding better results after frozen/thawed transfers, and a reduction in the number of embryos transferred, which generates fewer pregnancies with the fresh transfers and less multiple births. Slowly but consistently, centers in Latin America are transferring fewer embryos and therefore looking at cumulative pregnancy and delivery rates (fresh plus frozen), as a better index of success than fresh transfer alone. As expected, the proportion of cycles with FET is higher in younger women. Thus, 15,833 transfers (35.2%) were performed in women ≤ 34, 10,441 (35%) in women 35-39 years and only 3,517 (11.8%) in women ≥ 40. The CPR/ET has increased throughout these 15 years in every age categories (Fig 22). It is worth noting that CPR almost doubled in women ≤ 34 (16 to 30%), and it is also important to consider that RLA registers the age of women at the time of transfer, not at the time of embryo freezing. The DR/ET with at least one live birth increased from 13% in 1995 to 19% in 2009 (Fig 23).
MULTIPLE GESTATION / BIRTHS
Between 1995 and 2009 and consistent with a reduction in the mean number of embryos transferred, the proportion of women with multiple gestations decreased from 27 to 21%. The proportion of twin pregnancies has remained unchanged, but high order multiples have dropped from 8 to 2% in these 15 years (Fig 24). In women under 35, the reduction in the mean number of embryos transferred from 3.6 (1995) to 2.4 (2009) had a great impact in the frequency of pregnancies with triplets and more, which dropped from 10% in 1995 to 2% in 2009. However, the frequency of twin pregnancy remained unchanged in 23% (Fig 25). In this age group, the elective transfer of two embryos (eDET) decrease the rate of high order to only 0.3%, but twin pregnancies remains in 25 to 26% (Fig 25b). This high proportion of twin pregnancies is most likely the result of a sub-selection of a cohort of more fertile women having a larger number of good quality embryos at the time of transfer.
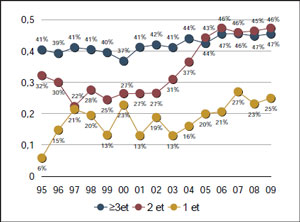
Figure 20. Clinical pregnancy rate according to the number of embryos transferred in Oocyte Donation (OD). RLA, 1995-2009.
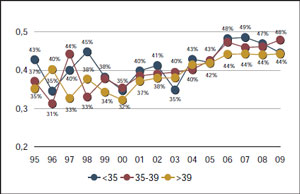
Figure 21. Clinical pregnancy rate according to age of recipient in Oocyte Donation (OD). RLA, 1995-2009.
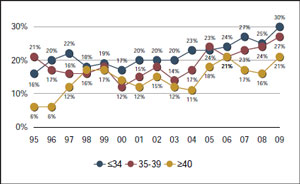
Figure 22. Clinical pregnancy rate according to age of female partner in Frozen embryo transfer (FET). RLA, 1995-2009.
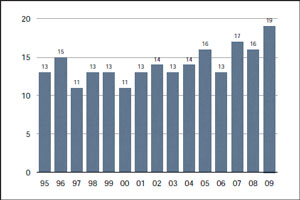
Figure 23. Live birth delivery rate by embryo transfer in Frozen embryo transfer (FET). RLA, 1995-2009.
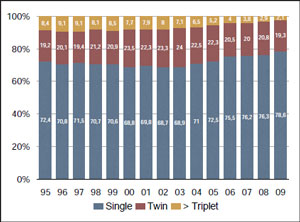
Figure 24. Multiple gestation in fresh autologous IVF/ICSI. RLA, 1995-2009.
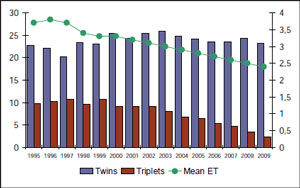
Figure 25a. Mean number of embryos transferred and multiple gestation in women ≤34. RLA, 1995-2009.
In 1990, the proportion of births with twins, triplets and quadruplets and more was 18, 7 and 2.5% respectively. Twenty years later, the proportion of twins has remained high (21%) but there has been a consistent drop in the occurrence of high order multiple births, with, 2% triplets and 0.1% of quadruplets.
Consequently, the proportion of babies born multiples is as follows. In 1990, almost half of babies born were multiples. Today 39.5% of babies are multiples; of these, 34% are born twins, 5% triplets and 0.4% quadruplets and more (Fig 26).
SPONTANEOUS ABORTION AND MALFORMATIONS
Spontaneous abortion.
Overall the rate of abortion in women undergoing ART between 1995 and 2009 was 19% (15,298 spontaneous abortions and 209 induced abortions); and varied according to the type of treatment. It was 23% in pregnancies after frozen embryo transfers, 19% in fresh autologous IVF/ICSI, and 17% in oocyte recipient. These differences are highly significant. (p < 0.0001).Chromosomal analysis was reported in 6% (921 cases) of spontaneous abortions, and among them, 35.7 % had one or more chromosome abnormalities, which are described in Table II. It is difficult to interpret this data. One possibility is that the low percentage of chromosomal abnormalities is due to sub registration; another possibility is that women treated with ART have many other causes for abortion apart from chromosomal aneuploidies, which are responsible for the majority of abortions in the general population.
Malformations
As in all other ART registries there are major difficulties in registering malformations. This is in part due to incomplete follow up of clinical pregnancies and also the absence of fixed criteria to evaluate and define anomalies in neonates or later in their lives. Bearing in mind all these difficulties, the RLA has encouraged the registration of this condition and out of 79,922 babies born; there is a clinical report in 22,085 babies (27.6%). In this group 372 clinical malformations were observed which represents a crude ratio of 1.7%. Table III represents the relative proportion of major malformations in babies generated by IVF, ICSI, cryopreservation, assisted hatching and OD. Malformation rate in babies born after OD is lower than fresh autologous IVF/ICSI.
NEONATAL OUTCOME: PRETERM DELIVERY AND PERINATAL MORTALITY
The RLA registers the weight and gestational age at birth as well as the percentage of live births stillbirths and early neonatal deaths.
Preterm delivery
Preterm delivery, defined as birth before 37 weeks pregnancy, increased over time reaching 20% in 1995 and 26% in 2009. In 1995, 8% of singletons were born before 37 weeks pregnancy, and 14% in 2009; in twin pregnancies, preterm birth increased from 35% (1995) to 61% (2009); in triplets it increased from 81% (1995) to 93%(2009); and as expected, quadruplets reached 100% in 2009.The main risk factor for preterm delivery is gestational order. Out of 47,173 deliveries with singletons, 14.9% were preterm, 58 % of twin births were preterm with a risk ratio of 3.8 (confidence interval 3.7-3.9; p<0.0001). Out of 998 triple deliveries, 90% were preterm, with a risk ratio of 6.0 (confidence interval 5.7-6.4; p<0.0001); and quadruplets had a risk ratio of 5.8 (confidence interval 4.7-7.1; p<0.0001) (Table IV).Especially important, is the significant increase in the frequency of very preterm delivery, defined as birth before 32 weeks gestation. Compared to singletons, who had a frequency of very preterm delivery of 2%; twins had a risk ratio of 3.2 (confidence interval 3.0-3.5; p p<0.0001); triplets had a risk ratio of 9.9 (confidence interval 9.2-10.7 p<0.0001); and quadruplets had a risk ratio of 21.7 (confidence interval 19.4-24.4 p<0.0001).
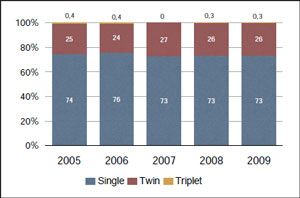
Figure 25b. Multiple gestation with eDET in women ≤34. RLA, 2005-2009.
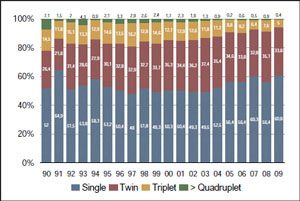
Figure 26. Proportion of babies born as singletons, twins, triplets and ≥ Quadruplets, by year. RLA, 1990-2009.
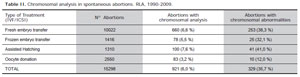
Table II. Chromosomal analysis in spontaneous abortions. RLA, 1990-2009.Type of Treatment (IVF/ICSI)Nº AbortionsAbortions with chromosomal analysisAbortions with chromosomal abnormalitiesFresh embryo transfer10022660 (6,6 %)253 (38,3 %)Frozen embryo transfer141678 (5,5 %)25 (32,1 %)Assisted Hatching1310100 (7,6 %)41 (41,0 %)Oocyte donation255083 (3,2 %)10 (12,0 %)TOTAL15298921 (6,0 %)329 (35,7 %)
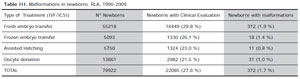
Table III. Malformations in newborns. RLA, 1990-2009.Type of Treatment (IVF/ICSI)Nº NewbornsNewborns with Clinical EvaluationNewborns with malformationsFresh embryo transfer5521816449 (29,8 %)312 (1,9 %)Frozen embryo transfer50931330 (26,1 %)18 (1.4 %)Assisted Hatching57501324 (23,0 %)11 (0,8 %)Oocyte donation138612982 (21,5 %)31 (1,0 %)TOTAL7992222085 (27,6 %)372 (1,7 %)
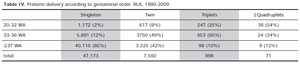
Table IV. Preterm delivery according to gestational order. RLA, 1990-2009.SingletonTwinTriplets≥Quadruplets20-32 WA1,172 (2%)617 (8%)247 (25%)38 (54%)33-36 WA5,891 (12%)3750 (49%)653 (65%)24 (34%)≥37 WA40,110 (85%)3,225 (42%)98 (10%)9 (12%)total47,1737,59299871
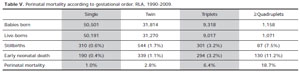
Table V. Perinatal mortality according to gestational order. RLA, 1990-2009.SingleTwinTriplets≥QuadrupletsBabies born50,50131,8149,3181,158Live-borns50,19131,2709,0171,071Stillbirths310 (0.6%)544 (1.7%)301 (3.2%)87 (7.5%)Early neonatal death190 (0.4%)339 (1.1%)294 (3.2%)130 (11.2%)Perinatal mortality1.0%2.8%6.4%18.7%
Perinatal Mortality
Associated to the increase in preterm delivery, plurality was strongly associated to perinatal mortality. In 50,501 babies born singletons, perinatal mortality was 10‰, which increased to 28‰ in almost 32,000 babies born twins, and 64‰ in 9,318 babies born triplets Thus, compared with singletons, twins had a risk ratio of 2.8 (confidence interval 2.5-3.1; p<0.0001); triplets had a risk ratio of 6.4 (confidence interval 5.8-7.1; p<0.0001); and quadruplets had a risk ratio of 18.9 (confidence interval 16.9-21.1; p<0.0001) (Table V).