JBRA Assisted Reproduction 2015;19(1):33-35
OPINION ARTICLE
doi: 10.5935/1518-0557.20150009
The stem cell research and the aging of Brazilian population
1Department of Hematology, HEMOPI-Centro de Hematologia e Hemoterapia do Piauí, Teresina, PI, Brasil 2Graduate School of Life and Environmental Sciences, University of Tsukuba, Ibaraki, Japan.
CONFLICT OF INTERESTS
No conflict of interest have been declared.
ABSTRACT
The developing countries are experiencing a shift in the population profile, faster than that experienced by developed countries, especially due to the consolidation of health practices and technological advances. These social changes also imply new socioeconomic models, able to escort social demands caused by the growth of the elderly population and the decrease in young economically active population. Several countries seek for actions that do not marginalize the elderly, and invest heavily in new technologies to ensure health access and active participation of this group in society. Stem cell research may reflect at an improvement of public health, reduction in costs of hospitalization and lead to prevention and treatment of extremely debilitating illness, like the neurodegenerative diseases. Preserving the physical and mental functional capacity is of extreme importance to ensure the active participation of elderly population in society.
Keywords: Stem cells, demographic aging, health public policy, support of research, neurodegenerative diseases.
The world is aging. It represents a victory of development, since this process is due to better nutrition, sanitation, health services and education. But celebration might be postponed, since new challenges are arising: decrease in economically active population and increase in age-related diseases.
Brazil has experienced a demographic revolution in the last century. The average life expectancy grew from 33.5 years during the 20th century to 76.5 years for women and 69 years for men by 2009, according to the Brazilian Institute of Geography and Statistics (IBGE, 2011). From 1999 to 2009 the elderly population increased from 9.1% to 11.3%, where individuals over 89 years old reached 47.8% of the total elderly population.
The change in the age profile of the Brazilian population forced the society to review and renew public policies and social organizations. Two major changes are the postponement of the retirement age and the establishment of special health care for elders. It is a common fact that among Brazilians, elderly have become an active part of the country’s economic and social development. Around 87% of the elderly men are heads of the families and they still actively contribute to the family income (Minayo, 2012).
Despite the increase in life expectancy and advances in social care, Brazil faces a serious challenge concerning their elders: to promote health and independence in a group with a high incidence of debilitating diseases. The treatment for individuals over 80 years old demands three times more financial resources. In addition, several geriatric diseases cause irreversible injuries that also raise financial demand of elderly health care (Veras, 2009). In 40 years the causes of mortality in Brazilian changed from young related causes to a group of complex and expensive diseases, similar to countries with older population (Gordilho et al., 2000; Lima-Costa & Veras, 2003; Veras, 2009). Nevertheless, the aging of the Brazilian population and other developing countries is happening faster than the process experienced previously by developed countries, therefore old policies might no longer be applicable.
The ways societies face aging process are varied, especially if we compare the traditional and nomad societies to the modern labor-based societies. In traditional societies, the elderly have chance to participate in the community; such as sharing their experience and knowledge verbally and taking care of the youngsters. Whereas, modern labor-based societies tend to exclude their elderly from the community once they reach the retirement age, regardless the potential they still possess. This immediate removal also neglects the fact that there is a possible psychological damage due to isolation and the feeling of worthlessness (Glass, 2003).
Elderly having an active role (paid or unpaid) in society is a common factor for a successful aging. Under the biomedical and psychosocial concept, a successful aging could be defined by three main perspectives: 1) low probability to diseases and disabilities related to them; 2) high physical and cognitive capacity; and 3) proactive attitude towards life, closely related to self-esteem and positive self-hated health evaluation (Glass, 2003; Teixeira el al., 2008).
Self-rated health is another tool for evaluation of health status, since it reflects an integrated perception by the individual that includes biological, psychosocial, and social dimensions (Jylha et al., 1998). Nevertheless, self-rated health is heavily influenced by socioeconomic conditions. (Lima-Costa et al., 2005). According to a qualitative study among elderly women in a small community in Brazil, measurement of the severity and relevance of health problems were determined more by the ability to deal with problems than by the problems themselves. Independence is, therefore, directly related to health perception, family support, access to medical care, and an active role in community (Lima-Costa et al., 2003).
To overcome the biomedical challenges of population aging, new therapeutic approaches are required and, among them, stem cell research has been showing astonishing results. Initially directed to hematopoietic transplantation, stem cell research has developed several other investigation goals, highlighted here two specifically: regenerative medicine and drug development. Table 1 summarizes current clinical trials in USA applying stem cell based therapies.
The regenerative medicine is focused restoring injured organ and tissue by replacing damaged cells for new ones grown in vitro. It aims to restore tissue structure and function, minimizing the use of prosthesis and the continuous need for medicine intake. But stem cell investigation has led to even further discoveries, like the anti-inflammatory properties of some populations of stem cells (Broughton et al., 2012). These stem cells regulate inflammatory processes and have shown exciting results in animal models of degenerative diseases, including neurodegenerative diseases, such as Parkinson’s and Alzheimer’s disease (AD). Therefore, it is hypothesize the possibility of isolating stem cell’s biomolecules for the formulation of new drugs or using a specific stem cell variety as a live medicine itself. For example, in mice with AD model the use of amniotic epithelial and mesenchymal cells showed the property to decrease chronic inflammation due to over reaction of microglial cells to amyloid beta molecule, the main responsible to the development of the disease. On the other hand, these stem cells were able to activate microglial cells in a controlled way to remove properly amyloid beta molecule and restore brain function. It’s important to focus the restoration of brain function, especially because the traditional drug therapy can only retard AD progress (Xue et al., 2011).
Several countries are already investing massively in stem cell research in order to face the new public health obstacles derived from population aging. Japan plans to invest $800 million in the induced pluripotent stem cell research at the Center for iPS Cell Research and Application, at Kyoto University. Since 2005, the US has invested an average of $375 million yearly only at the State of California. Meanwhile, Brazil’s investments is about $13,7 million yearly (Sipp, 2011; Trounson, 2012).
All these investments aren’t done aiming only at science development, they have solid economic motivation. It was estimated that 35 million people worldwide were living with some untreatable neurodegenerative disease in 2013, over a cost of $700 billion. Australia has 300.000 patients with AD and they cost annually $4.9 billion every year in medical expenses. In 2020 the number of patients is expected to reach 400.000. It’s hypothesized that a stem cell therapy that could reduce this number in 2.5% would pay itself (Dolgin, 2010). It is also important to highlight that initial technologies can be expensive and difficult but, as the knowledge is shared and studies evolve, cheaper and easier techniques are developed. We can cite the development of induced pluripotent stem cell and the spread of adult stem cell therapies.
Ageing is a process that does not need to be associated with the progress of health loss and degenerative diseases, as long as we can not only cure diseases but also avoid their progress from the beginning. A longer and healthy life, aligned to technology and the possibility to reproduce in advanced age (Biazotti et al., 2000; Vasconcelos et al, 2009; Carvalho & Leal, 2010), will extend youth and allow a productive and healthy senescence. Indeed, the concepts of youth and senescence will have to be reshaped.
Ignoring the elderly population needs can lead to a future pressure on the social welfare and public health system, among other services. It is crucial to invest in policies which promote life quality, prevent and minimize aging effects, in several social and technological contexts (Schoeni, 2005), thus elderly can stay independent with a preserved functional capacity and active roles in society.
The aging in Brazilian population is happening fast, now is the time to act and prepare society for the upcoming changes, while the country has higher proportion of economically active population and economy in expansion. These ideal conditions are not likely to remain much longer and losing this opportunity may represent a setback in the progress achieved so far.
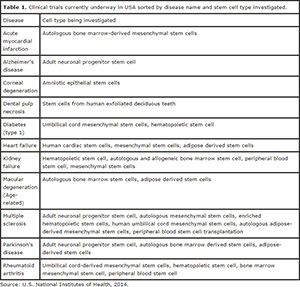
Table 1. Clinical trials currently underway in USA sorted by disease name and stem cell type investigated.
REFERENCES
Broughton BR, Lim R, Arumugam TV, Drummond GR, Wallace EM, Sobey CG. Post-stroke inflammation and the potential efficacy of novel stem cell therapies: focus on amnion epithelial cells. Front Cell Neurosci. 2013; 6:66.
Medline Crossref
Carvalho BF, Leal ESS. Influencia da morfologia do oócito em procedimentos de injeção intracitoplasmática de espermatozoide. Monograph. Faculty of Health, Social Sciences and Technology of Piauí – NOVAFAPI. Teresina, 2010.
Medline Crossref
Dolgin E. Gap in stem cell funding could drive Australian brain drain. Nat Med. 2010; 16:834
Medline Crossref
Glass TA. Assessing the success of successful aging. Ann Intern Med. 2003; 139:382-3.
Medline Crossref
Gordilho A, Nascimento JS, Ramos LR, Freire MPA, Espindola N, Maia R, Veras R, Karsch U., eds. Desafios a serem enfrentados no terceiro milênio pelo setor saúde na atenção integral ao idoso. Rio de Janeiro: UnATI/ UERJ; 2000.
Medline Crossref
IBGE - Brazilian Institute of Geography and Statistics. Demographic Census 2010. Available at
Medline Crossref
Jylha M, Guralnik JM, Ferrucci L, Jokela J, Heikkinen E. Is self-rated health comparable across cultures and genders? J Gerontol B Psychol Sci Soc Sci. 1998; 53:S144-52.
Medline Crossref
Lima-Costa MF, Veras RP. Saúde pública e envelhecimento. Cad Saude Publica. 2003; 19:700-1.
Lima-Costa MF, Barreto SM, Firmo JOA, Uchôa E. Socioeconomic position and health in a population of Brazilian elderly: The Bambuí Health and Ageing Study (BHAS). Rev Panam Salud Publica 2003; 13:387-94.
Medline Crossref
Lima-Costa MF, Firmo JOA, Uchoa E. Differences in self-rated health among older adults according to socioeconomic circumstances: the Bambuí Health and Aging Study. Cad. Saúde Pública. 2005; 21;830-9.
Medline Crossref
Minayo MCS. Aging of the Brazilian population and challenges for the health sector. Cad. Saúde Pública. 2012;28:208-9.
Medline Crossref
Schoeni RF, Martin LG, Andreski PM, Freedman VA. Persistent and growing socioeconomic disparities in disability among the elderly: 1982-2002. Am J Public Health. 2005;95:2065-70.
Medline Crossref
Sipp D. Global challenges in stem cell research and the many roads ahead. Neuron. 2011;70:573-6
Medline Crossref
Teixeira INDO, Neri AL. Successful aging: a goal in the course of life. Psicol. USP. 2008; 19:81-94.
Crossref
Trounson A. California institute for regenerative medicine: accelerating stem cell therapies in California and beyond. Stem Cells. 2012; 30:357-9.
Medline Crossref
Veras R. Envelhecimento populacional contemporâneo: demandas, desafios e inovações. Rev. Saúde Pública. 2009, 43:548-54
Crossref
Xue SR, Chen CF, Dong WL, Hui GZ, Liu TJ, Guo LH. Intracerebroventricular transplantation of human amniotic epithelial cells ameliorates spatial memory deficit in the doubly transgenic mice coexpressing APPswe and PS1ΔE9-deleted genes. Chin Med J (Engl). 2011;124:2642-8.
Medline