JBRA Assist. Reprod. 2018;22(3):215-220
ORIGINAL ARTICLE
doi: 10.5935/1518-0557.20180043
Are age and anti-Müllerian hormone good predictors of ovarian reserve and response in women undergoing IVF?
1IBRRA - Brazilian Institute of Assisted Reproduction, Belo Horizonte, Brazil.
2Department of Reproductive Medicine, Hôpital Jean Verdier (AP-HP), University Paris XIII, and INSERM, Paris, France.
3School of Medicine, Tecnologico de Monterrey and Center for Reproductive Medicine CREASIS, San Pedro Monterrey, Mexico.
CONFLICTS OF INTEREST
The authors have no conflict of interest to declare.
ABSTRACT
Objective: Ovarian reserve evaluation has been the focus of substantial clinical research for several years. This study aimed to examine the associations between markers of ovarian reserve and ovarian response.
Methods: This prospective study included 132 infertile women aged 24-48 years undergoing routine exploration during unstimulated cycles prior to the start of assisted reproductive technology (ART) treatments at our center from July 2015 to January 2017. Descriptive parameters and patient characteristics were reported as mean (SD) or median (range) values depending on the data distribution pattern. Student’s t-test was performed for continuous variables; the Wilcoxon and Pearson’s test were used for data not following a normal distribution; and Fisher’s test was used for categorical variables. p<0.05 was considered statistically significant.
Results: At the time of the study, the patients had a mean age of 35.7±3.84 years. On day 3 of the cycle, the mean anti-Müllerian hormone (AMH) serum level was 2.84±1.57 ng/mL and the patients had 14.68±4.2 antral follicles (AFC). A significant correlation was observed between AMH and age (r=-0.34 p<.01), follicle stimulating hormone (FSH) serum levels (r=-0.32, p<.01), AFC (r=0.81, p<.00001), total dose of medication during ovarian stimulation (r=-0.28, p<.0003), and ongoing pregnancy rate (p<.05). Age was significantly correlated with FSH (r=0.46, p<.01), AFC (r=-0.34, p<.00001), total dose of medication during ovarian stimulation (r=0.43, p<.0003), and ongoing pregnancy rate (p<.04).
Conclusion: Serum AMH and age are independent predictors of ovarian reserve and ovarian stimulation outcome in infertile women. Age and serum AMH level may be used to advise subfertile couples of their pregnancy prospects.
Keywords: Age, anti-Müllerian hormone, antral follicle count, ongoing pregnancy
INTRODUCTION
Female fecundity begins to decrease after women reach the age of 30 years, primarily as a result of decreases in the proportion of normal eggs available as a consequence of a continuous process of oocyte atresia. Although all women experience decreases in fecundity, it is difficult to predict the pace of reproductive decline in each individual. The age-related decline in fecundity is characterized by decreases in both egg quality and number, in addition to population-based changes in the expression of markers of ovarian activity, such as gradual increases in circulating FSH and decreases in circulating anti-Müllerian hormone (AMH) and inhibin B levels.
A classic report on the effects of female age on fertility found that the proportion of women off contraceptives unable to get pregnant increased steadily according to their age at the time of marriage: 6% at the ages of 20-24 years; 9% at the ages of 25-29 years; 15% at the ages of 30-34 years; 30% at the ages of 35-39 years; and 64% at the ages of 40-44 years (Menken et al., 1986). The age-associated decline in female fecundity and increase in risk of miscarriage have been largely ascribed to oocyte abnormalities. The meiotic spindle in the oocytes of older women frequently exhibits abnormalities in chromosome alignment and microtubular matrix composition (Battaglia et al., 1996). Higher rates of single chromatid abnormalities in oocytes (Angell, 1994), as well as aneuploidy in preimplantation embryos (Benadiva et al., 1996) and ongoing pregnancies, have been observed in older women. The higher rate of aneuploidy is a major cause of increased miscarriage and decreased live birth rates in women of advanced reproductive age.
Ovarian reserve evaluation has been the focus of substantial clinical research for several years (Navot et al., 1987; Hofmann et al., 1996; Toner et al., 1991; Frattarelli et al., 2000; Scott & Hofmann, 1995). Anti-Müllerian hormone (AMH), also known as Müllerian inhibiting substance, is a dimeric glycoprotein belonging to the transforming growth factor-b (TGF-b) superfamily, whose members include activins and inhibins, produced exclusively in the gonads, as shown more than two decades ago in animals (Vigier et al., 1984) and later in humans (Rey et al., 2003; di Clemente et al., 1992). In women, AMH is synthesized in the granulosa cells (GC) surrounding preantral and small antral follicles (Weenen et al., 2004; Durlinger et al., 2002). Despite the use of ultrasensitive assays, AMH is barely detectable in serum at birth. It reaches higher levels after puberty (Guibourdenche et al., 2003; Rajpert-De Meyts et al., 1999) and then declines with aging, until it becomes undetected again at menopause (La Marca et al., 2005). Although the physiological roles of AMH and the mechanisms involved in the regulation of the hormone are still poorly established, recent studies have singled AMH out as an attractive marker for assessing of ovarian activity. Baseline AMH, determined before stimulation (usually on day 3 of the cycle), was found to be a better measure of decreased ovarian reserve than classic parameters such as increases in follicle stimulating hormone (FSH) levels or decreases in inhibin B and antral follicle count (de Vet et al., 2002; Fanchin et al., 2003; 2005; Muttukrishna et al., 2005; Tremellen et al., 2005; Hazout, 2006). An inverse correlation was described between AMH and baseline FSH levels (Piltonen et al., 2005), in addition to age.
In assisted reproductive technology (ART), serum AMH has been described as a more reliable hormonal marker of ovarian response to controlled ovarian hyperstimulation (COH) with gonadotropins than baseline FSH, estradiol, inhibin B or female patient age (Anckaert et al., 2012; Hazout et al., 2004; Muttukrishna et al., 2004; Nardo et al., 2009; Peñarrubia et al., 2005; Seifer et al., 2002). AMH has also been claimed to possess at least the same level of accuracy as the antral follicle count (AFC) as a predictor of poor (Broer et al., 2009) and excessive (Broer et al., 2011) response. In addition, high serum AMH levels before the start of COH have been associated with increased risk of ovarian hyperstimulation syndrome (OHSS) (Lee et al., 2008; Nelson et al., 2007). As with other ovarian reserve tests, AMH is not a good predictor of embryo quality or pregnancy in COS cycles, suggesting that AMH is a marker of quantitative rather than qualitative aspects of ovarian reserve (Rey et al., 2003; Anckaert et al., 2012; Broer et al., 2011; Nelson et al., 2007; Smeenk et al., 2007). However, age has been described as a good predictor of embryo quality (Scheffer et al., 2017a).
The aim of the present study was to investigate and compare the correlations of AMH and age with prognostic parameters and outcomes of assisted reproductive technology (ART) treatment.
MATERIAL AND METHODS
Subjects
This prospective study included 132 infertile women aged 24-48 years undergoing routine exploration during unstimulated cycles prior to the start of assisted reproductive technology (ART) treatments at our center from July 2015 to January 2017. Enrolled patients met the following inclusion criteria: i) both ovaries present; ii) no current or past diseases affecting the ovaries or gonadotropin/sex steroid secretion, clearance, or excretion; iii) no current hormone therapy; iv) adequate visualization of the ovaries on transvaginal ultrasound scans; and v) total number of small antral follicles (3-12 mm in diameter) between 1 and 32 in both ovaries. All patients signed an informed consent form prior to inclusion in the study.
Protocol
The patients were given leuprolide acetate (Lupron, Abbott, France). The GnRH-agonist was initiated at a dose of 2.0 mg/day during the mid-luteal phase, overlapping with approximately five days of oral contraceptive pill (OCP) administration (Diane 35, Schering, Brazil). Pituitary down-regulation was monitored and patients with adequate pituitary desensitization were started on a recombinant FSH regime (Gonal-F; Merck-Serono Pharmaceuticals, Italy) and the dose of GnRH-agonist was reduced to 1.0 mg/day. FSH was started with dosages between 150 and 300 IU/day for four days with or without human menopausal gonadotropin (hMG) (Menopur; Ferring Pharmaceuticals, Germany) based on AFC and AMH. Thereafter, the dose of FSH was individually adjusted according to estradiol (E2) response and vaginal ultrasound findings.
When two follicles reached a size ≥ 16-18 mm, 250 mg of recombinant human Chorionic Gonadotropin (Ovidrel, Merck-Serono Pharmaceuticals, Italy) were administered and oocyte retrieval occurred 35 to 36 hours later.
Intracytoplasmic sperm Injection (ICSI) was routinely performed in all fertilization procedures as described in the literature (Palermo et al., 1992). Fertilization was evident when two pronuclei were observed. Embryos were cultured until the day of transfer (day 3) in IVF Global® media (Life Global, Canada) supplemented with 10% synthetic serum substitute (SSS) and graded according to the criteria described by Veeck (1999) and Hsu et al. (1999) before transfer.
The number of embryos to be transferred was defined based on the guidelines published by the Brazilian Federal Board of Medicine (CFM).
Luteal phase support was achieved with micronized P4, 600 mg/day, administered continuously by vaginal route, starting on the evening of ET.
Ongoing pregnancy (OP) was assessed as biochemical pregnancy (BQ) and subsequent observation of one or more gestational sacs. Miscarriage was defined as a clinically recognized pregnancy loss occurred before 20 weeks of gestation.
Hormone Measurements and Ultrasound Scans
On day 3 of the cycle preceding COH, the female patients had blood samples harvested by venipuncture to have their serum AMH and FSH levels measured, and had their follicles measured by transvaginal ultrasound.
AMH and FSH serum levels were determined using an automated multi-analysis system with chemiluminescence detection (ACS-180; Bayer Diagnostics, Puteaux, France). Serum AMH levels were determined using a second-generation enzyme-linked immunosorbent assay. Intra- and inter- assay coefficients of variation (CV) were <6% and <10%, respectively, with lower detection limit at 0.13 ng/ mL and linearity up to 21 ng/mL for AMH.
For FSH testing, functional sensitivity was 0.1 mIU/mL, and the intra- and inter-assay CV were 3% and 5%, respectively.
A single operator blinded to the hormone assay results performed the ultrasound examinations using a 3.7-9.3 MHz multi-frequency transvaginal probe (RIC5-9H; General Electric Medical Systems, Paris, France). The objective of ultrasound examination was to evaluate the number and size of small antral follicles. Follicles with mean diameters of 3-12 mm (mean of two orthogonal diameters) in both ovaries were considered. To optimize the reliability of ovarian follicular assessment, the ultrasound scanner was equipped with a tissue harmonic imaging system (Thomas & Rubin, 1998), which yielded improved image resolution and adequate recognition of follicular borders. Intra-analysis CV for follicular and ovarian measurements were <5%, and their lower limit of detection was 0.1 mm. In an effort to evaluate the bulk of granulosa cells in both ovaries, we calculated the mean follicle diameter (cumulative follicle diameter divided by the number of follicles measuring 3-12 mm in diameter in both ovaries) and the largest follicle diameter.
Ethical approval
Written informed consent was obtained from all participants before inclusion in the study. The Ethics Committee of the Brazilian Institute of Assisted Reproduction approved the study
Statistical Analysis
Descriptive parameters and patient characteristics were reported as mean (SD) or median (range) values depending on variable distribution.
Student’s t-test and the Wilcoxon signed-rank test were performed for continuous variables; Fisher's exact test was performed for categorical variables; and Pearson's correlation coefficient was calculated.
p<0.05 was considered statistically significant.
RESULTS
At the time of the study, the 132 patients included had a mean age of 35.7±3.84 years, a BMI of 22.30±1.78 kg/m2, and a length of infertility of 2.66±2.03 years. On cycle day 3, the mean serum AMH level was 2.84±1.57ng/mL. At baseline, the patients had 14.68±4.2 antral follicles.
AMH was significantly correlated with age (r=-0.34 p<.01) (Figure 1), FSH (r=-0.32, p<.01), AFC (r=0.81, p<.00001), total dose of ovarian stimulation medication (r=-0.28, p<.0003), miscarriage rate (p<.02), and ongoing pregnancy rate (p<.05) (Figure 2).
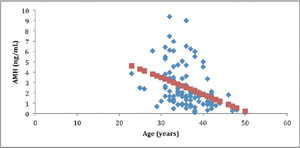
Figure 1. Correlation between anti-Müllerian hormone (AMH) and age
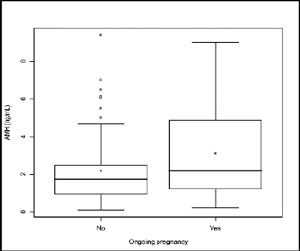
Figure 2. Comparison between serum anti-Müllerian hormone (AMH) levels of infertile patients with ongoing pregnancies and infertile patients without ongoing pregnancies. The box represents the interquartile range containing 50% of the values. The whiskers are lines that extend from the box to the highest and lowest values, excluding outliers. A line across the box indicates the median. p<.05, Student’s t-test
Age was significantly correlated with FSH (r=0.46, p<.01), AFC (r=-0.34, p<.00001), total dose of ovarian stimulation medication (r=0.43, p<.0003), miscarriage rate (p<.03), an and ongoing pregnancy rate (p<.04) (Figure 3).
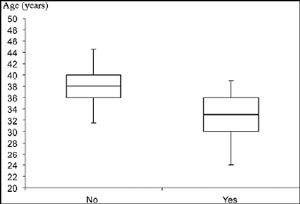
Figure 3. Comparison between the ages of infertile patients with ongoing pregnancies and infertile patients without ongoing pregnancies. The box represents the interquartile range containing 50% of the values. The whiskers are lines that extend from the box to the highest and lowest values, excluding outliers. A line across the box indicates the median. p<.05, Student’s t-test
DISCUSSION
This study demonstrated that serum AMH level and age were independent predictors of ovarian reserve and ovarian stimulation outcome in infertile women. Ovarian reserve is currently defined as the interplay between the quantity and quality of the follicles left in the ovary, and several proxy variables for pool size have been well described in the literature. Female reproductive aging is a process dominated by the gradual decline of oocyte quantity and quality (te Velde & Pearson, 2002). With increasing chronological age, female fecundity decreases (Broekmans et al., 2009). Progressive follicle decline is accompanied by notable changes in menstrual cycle regularity, with menopause as the final step in the ovarian aging process (Faddy et al., 1992; Hansen et al., 2008; Wallace & Kelsey, 2004).
Age has been used as a predictor of the number of harvested oocytes, number of metaphase II oocytes, and embryo quality. This marker of ovarian reserve is the single best predictor of reproductive outcome in women, and oocyte is the locus of reproductive aging in women. Whole chromosomal nondisjunction and precocious sister chromatid separation have been correlated to maternal aging. Disturbance in sister chromatid cohesion might be a causal mechanism predisposing to premature chromatid separation and subsequently to nondisjunction in female meiosis. In addition, the asymmetry of female meiosis division might favor nonrandom meiotic segregation of chromosomes and chromatids.
Oocyte aging leads to increased mitochondrial DNA damage and decreased oxidative phosphorylation and ATP production. Mitochondrial mutations in follicular cells surrounding the oocytes have been correlated with maternal age, suggesting that oxidative phosphorylation in the follicle is compromised (Smeenk et al., 2007). Anti-Müllerian hormone has been correlated with increased miscarriage rates. This finding is surprising, since decreased quantitative ovarian reserve is considered to be a reflection of advanced ovarian aging, a variable clearly associated with increased rates of fetal aneuploidy and miscarriage (Levi et al., 2001; Elter et al., 2005; Lekamge et al., 2007). The correlations described in the literature between AMH serum levels and pregnancy rates (PR) after reproductive therapies such as IVF were not conclusive. Some authors (Lekamge et al., 2007; Peñarrubia et al., 2005; Fiçicioglu et al., 2006; Laven et al., 2004) were unable to find a correlation between baseline AMH levels and pregnancy rates, whereas others (Broer et al., 2011; Laven et al., 2004; Eldar-Geva et al., 2005) observed an association between higher baseline serum AMH levels and higher clinical PR. Similarly, a study described a positive correlation between embryo scores and serum AMH levels at the time of hCG administration (Silberstein et al., 2006), while another group of authors, in a more recent study (Lekamge et al., 2007), found no correlation between serum AMH on day 3 of a control cycle and embryo morphology. A study reported a significant association between serum AMH measured on the first day of a COH cycle and treatment outcome (pregnancy) using a cutoff level for negative predictive value (Fréour et al., 2006). Data heterogeneity hampers further comparisons between published findings.
In our study, total consumption of gonadotropins was statistically correlated with AMH and age. The relationship between serum AMH levels and controlled ovarian stimulation outcome observed in this study is in agreement with previous studies on serum AMH levels. Serum AMH seems to reflect the follicular pool, and its production is independent of the gonadotropin-dependent indicators of ovarian reserve (Seifer et al., 2002; van Rooij et al., 2002; Scheffer, 2017b).
An ideal ovarian reserve test should be reproducible, with limited inter- and intra-cycle variability, and highly specific to minimize the risk of incorrectly categorizing women as having decreased ovarian reserve. No measure of ovarian reserve is perfect; however, AMH level and age have yielded good predictive value. More studies are needed to improve the accuracy and interpretation of the current ovarian reserve markers to clearly define cut-off levels for each marker and find other markers more strongly correlated with the number of ova retrieved, embryo quality, and clinical pregnancy rates. Determining the etiology of maternal aging on oocyte competence might improve patient care and fertility treatment outcomes.
CONCLUSION
Serum AMH level and age are predictors of ovarian reserve and ovarian stimulation outcome in infertile women. Age and serum AMH levels might be used to advise subfertile couples of their pregnancy prospects. These markers should be deemed as an important element in the contemporary practice of reproductive medicine.
Acknowledgement
The authors would like to thank the Brazilian Institute of Assisted Reproduction for the financial support provided to this study.
REFERENCES
Anckaert E, Smitz J, Schiettecatte J, Klein B, Arce JC. The value of anti-Mullerian hormone measurement in the long GnRH agonist protocol: association with ovarian response and gonadotrophin-dose adjustments. Hum Reprod. 2012;27:1829-39.
Medline Crossref
Angell RR. Aneuploidy in older women. Higher rates of aneuploidy in oocytes from older women. Hum Reprod. 1994;9:1199-200.
Medline Crossref
Battaglia DE, Goodwin P, Klein NA, Soules MR. Influence of maternal age on meiotic spindle assembly in oocytes from naturally cycling women. Hum Reprod. 1996;11:2217-22.
Medline Crossref
Benadiva CA, Kligman I, Munne S. Aneuploidy 16 in human embryos increases significantly with maternal age. Fertil Steril. 1996;66:248-55.
Medline Crossref
Broekmans FJ, Soules MR, Fauser BC. Ovarian aging: mechanisms and clinical consequences. Endocrinol Rev. 2009;30:465-93.
Medline Crossref
Broer SL, Mol BW, Hendriks D, Broekmans FJ. The role of antimullerian hormone in prediction of outcome after IVF: comparison with the antral follicle count. Fertil Steril. 2009;91:705-14.
Medline Crossref
Broer SL, Dólleman M, Opmeer BC, Fauser BC, Mol BW, Broekmans FJ. AMH and AFC as predictors of excessive response in controlled ovarian hyperstimulation: a meta-analysis. Hum Reprod Update. 2011;17:46-54.
Medline Crossref
de Vet A, Laven JS, de Jong FH, Themmen AP, Fauser BC. Antimüllerian hormone serum levels: a putative marker for ovarian aging. Fertil Steril. 2002;77:357-62.
Medline Crossref
di Clemente N, Ghaffari S, Pepinsky RB, Pieau C, Josso N, Cate RL, Vigier B. A quantitative and interspecific test for biological activity of anti-müllerian hormone: the fetal ovary aromatase assay. Development. 1992;114:721-7.
Medline
Durlinger AL, Gruijters MJ, Kramer P, Karels B, Ingraham HA, Nachtigal MW, Uilenbroek JT, Grootegoed JA, Themmen AP. Anti-Müllerian hormone inhibits initiation of primordial follicle growth in the mouse ovary. Endocrinology. 2002;143:1076-84.
Medline Crossref
Eldar-Geva T, Ben-Chetrit A, Spitz IM, Rabinowitz R, Markowitz E, Mimoni T, Gal M, Zylber-Haran E, Margalioth EJ. Dynamic assays of inhibin B, anti-Mullerian hormone and estradiol following FSH stimulation and ovarian ultrasonography as predictors of IVF outcome. Hum Reprod. 2005;20:3178-83.
Medline Crossref
Elter K, Kavak ZN, Gokaslan H, Pekin T. Antral follicle assessment after down-regulation may be a useful tool for predicting pregnancy loss in in vitro fertilization pregnancies. Gynecol Endocrinol. 2005;21:33-7.
Medline Crossref
Faddy MJ, Gosden RG, Gougeon A, Richardson SJ, Nelson JF. Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Hum Reprod. 1992;7:1342-6.
Medline Crossref
Fanchin R, Schonäuer LM, Righini C, Guibourdenche J, Frydman R, Taieb J. Serum anti-Müllerian hormone is more strongly related to ovarian follicular status than serum inhibin B, estradiol, FSH and LH on day 3. Hum Reprod. 2003;18:323-7.
Medline Crossref
Fanchin R, Taieb J, Lozano DH, Ducot B, Frydman R, Bouyer J. High reproducibility of serum anti-Mullerian hormone measurements suggests a multi-staged follicular secretion and strengthens its role in the assessment of ovarian follicular status. Hum Reprod. 2005;20:923-7.
Medline Crossref
Fiçicioglu C, Kutlu T, Baglam E, Bakacak Z. Early follicular antimüllerian hormone as an indicator of ovarian reserve. Fertil Steril. 2006;85:592-6.
Medline Crossref
Frattarelli JL, Bergh PA, Drews MR, Sharara FI, Scott RT. Evaluation of basal estradiol levels in assisted reproductive technology cycles. Fertil Steril. 2000;74:518-24.
Medline Crossref
Fréour T, Mirallié S, Colombel A, Bach-Ngohou K, Masson D, Barrière P. Anti-mullerian hormone: clinical relevance in assisted reproductive therapy. Ann Endocrinol. 2006;67:567-74.
Medline Crossref
Guibourdenche J, Lucidarme N, Chevenne D, Rigal O, Nicolas M, Luton D, Léger J, Porquet D, Noël M. Anti-Müllerian hormone levels in serum from human foetuses and children: pattern and clinical interest. Mol Cell Endocrinol. 2003;211:55-63.
Medline Crossref
Hansen KR, Knowlton NS, Thyer AC, Charleston JS, Soules MR, Klein NA. A new model of reproductive aging: the decline in ovarian non-growing follicle number from birth to menopause. Hum Reprod. 2008;23:699-708.
Medline Crossref
Hazout A, Bouchard P, Seifer DB, Aussage P, Junca AM, Cohen-Bacrie P. Serum antimüllerian hormone/müllerian-inhibiting substance appears to be a more discriminatory marker of assisted reproductive technology outcome than follicle-stimulating hormone, inhibin B, or estradiol. Fertil Steril. 2004;82:1323-9.
Medline Crossref
Hazout A. [Quality of ovarian reserve: inhibin B on day 3 of the cycle or antimüllerian hormone (AMH)?] Gynecol Obstet Fertil. 2006;34:1001-2. In French.
Medline Crossref
Hofmann GE, Sosnowski J, Scott RT, Thie J. Efficacy of selection criteria for ovarian reserve screening using the clomiphene citrate challenge test in a tertiary fertility center population. Fertil Steril. 1996;66:49-53.
Medline Crossref
Hsu MI, Mayer J, Aronshon M, Lanzendorf S, Muasher S, Kolm P, Oehninger S. Embryo implantation in in vitro fertilization and intracytoplasmic sperm injection: impact of cleavage status, morphology grade, and number of embryos transferred. Fertil Steril. 1999;72:679-85.
Medline Crossref
La Marca A, De Leo V, Giulini S, Orvieto R, Malmusi S, Gianella L, Volpe A. Anti-Mullerian hormone in premenopausal women and after spontaneous or surgically induced menopause. J Soc Gynecol Invest. 2005;12:545-8.
Medline Crossref
Laven JS, Mulders AG, Visser JA, Themmen AP, De Jong FH, Fauser BC. Anti-Müllerian hormone serum concentrations in normoovulatory and anovulatory women of reproductive age. J Clin Endocrinol Metab. 2004;89:318-23.
Medline Crossref
Lee TH, Liu CH, Huang CC, Wu YL, Shih YT, Ho HN, Yang YS, Lee MS. Serum anti-Müllerian hormone and estradiol levels as predictors of ovarian hyperstimulation syndrome in assisted reproduction technology cycles. Hum Reprod. 2008;23:160-7.
Medline Crossref
Lekamge DN, Barry M, Kolo M, Lane M, Gilchrist RB, Tremellen KP. Anti-Mullerian hormone as a predictor for IVF outcome. Reprod Biomed Online. 2007;14:602-10.
Medline Crossref
Levi AJ, Raynault MF, Bergh PA, Drews MR, Miller BT, Scott RT Jr. Reproductive outcome in patients with diminished ovarian reserve. Fertil Steril. 2001;76:666-9.
Medline Crossref
Menken J, Trussell J, Larsen U. Age and infertility. Science. 1986;233:1389-94.
Medline Crossref
Muttukrishna S, Suharjono H, McGarrigle H, Sathanandan M. Inhibin B and anti-Mullerian hormone: markers of ovarian response in IVF/ICSI patients? BJOG. 2004;111:1248-53.
Medline Crossref
Muttukrishna S, McGarrigle H, Wakim R, Khadum I, Ranieri DM, Serhal P. Antral follicle count, anti-mullerian hormone and inhibin B: predictors of ovarian response in assisted reproductive technology? BJOG. 2005;112:1384-90.
Medline Crossref
Nardo LG, Gelbaya TA, Wilkinson H, Roberts SA, Yates A, Pemberton P, Laing I. Circulating basal anti-Müllerian hormone levels as predictor of ovarian response in women undergoing ovarian stimulation for in vitro fertilization. Fertil Steril. 2009;92:1586-93.
Medline Crossref
Navot D, Rosenwaks Z, Margalioth EJ. Prognostic assessment of female fecundity. Lancet. 1987;2:645-7.
Medline Crossref
Nelson SM, Yates RW, Fleming R. Serum anti-Müllerian hormone and FSH: prediction of live birth and extremes of response in stimulated cycles--implications for individualization of therapy. Hum Reprod. 2007;22:2414-21.
Medline Crossref
Palermo GP, Joris H, Devroey P, Van Steirteghem AC. Pregnancies after intracytoplasmatic injection of a single spermatozoon into an oocyte. Lancet. 1992;340:17-8.
Medline Crossref
Peñarrubia J, Fábregues F, Manau D, Creus M, Casals G, Casamitjana R, Carmona F, Vanrell JA, Balasch J. Basal and stimulation day 5 anti-Mullerian hormone serum concentrations as predictors of ovarian response and pregnancy in assisted reproductive technology cycles stimulated with gonadotropin-releasing hormone agonist--gonadotropin treatment. Hum Reprod. 2005;20:915-22.
Medline Crossref
Piltonen T, Morin-Papunen L, Koivunen R, Perheentupa A, Ruokonen A, Tapanainen JS. Serum anti-Müllerian hormone levels remain high until late reproductive age and decrease during metformin therapy in women with polycystic ovary syndrome. Hum Reprod. 2005;20:1820-6.
Medline Crossref
Rajpert-De Meyts E, Jørgensen N, Graem N, Müller J, Cate RL, Skakkebaek NE. Expression of anti-Müllerian hormone during normal and pathological gonadal development: association with differentiation of Sertoli and granulosa cells. J Clin Endocrinol Metab. 1999;84:3836-44.
Medline Crossref
Rey R, Lukas-Croisier C, Lasala C, Bedecarrás P. AMH/MIS: what we know already about the gene, the protein and its regulation. Mol Cell Endocrinol. 2003;211:21-31.
Medline Crossref
Scheffer JB, Scheffer BB, de Carvalho RF, Rodrigues J, Grynberg M, Mendez Lozano DH. Age as A Predictor of Embryo Quality Regardless of The Quantitative Ovarian Response. Int J Fertil Steril. 2017a;11:40-6.
Medline Crossref
Scheffer JB. Anti-Müllerian hormone - Marker of Female Reproductive Ageing and for Assessing Ovarian Function and Ovarian Stimulation Outcome. J Gynecol Women’s Health. 2017b;3:555624.
Crossref
Scott RT Jr, Hofmann GE. Prognostic assessment of ovarian reserve. Fertil Steril. 1995;63:1-11.
Medline Crossref
Seifer DB, MacLaughlin DT, Christian BP, Feng B, Shelden RM. Early follicular serum müllerian-inhibiting substance levels are associated with ovarian response during assisted reproductive technology cycles. Fertil Steril. 2002;77:468-71.
Medline Crossref
Silberstein T, MacLaughlin DT, Shai I, Trimarchi JR, Lambert-Messerlian G, Seifer DB, Keefe DL, Blazar AS. Mullerian inhibiting substance levels at the time of HCG administration in IVF cycles predict both ovarian reserve and embryo morphology. Hum Reprod. 2006;21:159-63.
Medline Crossref
Smeenk JM, Sweep FC, Zielhuis GA, Kremer JA, Thomas CM, Braat DD. Antimüllerian hormone predicts ovarian responsiveness, but not embryo quality or pregnancy, after in vitro fertilization or intracytoplasmic sperm injection. Fertil Steril. 2007;87:223-6.
Medline Crossref
te Velde ER, Pearson PL. The variability of female reproductive ageing. Hum Reprod Update. 2002;8:141-54.
Medline Crossref
Thomas JD, Rubin DN. Tissue harmonic imaging: why does it work? J Am Soc Echocardiogr. 1998;11:803-8.
Medline Crossref
Toner JP, Philput CB, Jones GS, Muasher SJ. Basal follicle-stimulating hormone level is a better predictor of in vitro fertilization performance than age. Fertil Steril. 1991;55:784-91.
Medline Crossref
Tremellen KP, Kolo M, Gilmore A, Lekamge DN. Anti-mullerian hormone as a marker of ovarian reserve. Aust N Z J Obstet Gynaecol. 2005;45:20-4.
Medline Crossref
van Rooij IA, Broekmans FJ, te Velde ER, Fauser BC, Bancsi LF, de Jong FH, Themmen AP. Serum anti-Müllerian hormone levels: a novel measure of ovarian reserve. Hum Reprod. 2002;17:3065-71.5
Medline Crossref
Veeck LL. An Atlas of Human Gametes and Conceptuses. New York: Parthenon; 1999.
Vigier B, Picard JY, Tran D, Legeai L, Josso N. Production of anti-Müllerian hormone: another homology between Sertoli and granulosa cells. Endocrinology. 1984;114:1315-20.
Medline Crossref
Wallace WH, Kelsey TW. Ovarian reserve and reproductive age may be determined from measurement of ovarian volume by transvaginal sonography. Hum Reprod. 2004;19:1612-7.
Medline Crossref
Weenen C, Laven JS, Von Bergh AR, Cranfield M, Groome NP, Visser JA, Kramer P, Fauser BC, Themmen AP. Anti-Müllerian hormone expression pattern in the human ovary: potential implications for initial and cyclic follicle recruitment. Mol Hum Reprod. 2004;10:77-83.
Medline Crossref