JBRA Assist. Reprod. 2019;23(4):361-366
ORIGINAL ARTICLE
doi: 10.5935/1518-0557.20190034
Spontaneous pregnancies in patients with at least one failed IVF cycle after the management of autoimmune disorders, hereditary thrombophilia, and methylation disorders
1Division of Perinatology, Department of Obstetrics and Gynecology, Hacettepe University, Ankara, Turkey
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.
ABSTRACT
Objective: This study aimed to describe the impact on achieving spontaneous pregnancy of treating patients with at least one failed in-vitro fertilization (IVF) cycle for autoimmune disorders, hereditary thrombophilia, and methylation disorders.
Methods: Fifty-three patients who met the enrollment criteria seen between January 2007 and October 2017 were included in this retrospective cohort study. The patients were retrospectively assessed for the presence of hereditary thrombophilia, methylenetetrahydrofolate reductase (MTHFR) polymorphisms, serum vitamin B12/folate/homocysteine levels, and autoimmune antibody positivity. The required data were extracted from the institutional patient database. Statistical analyses were performed on Statistical Package for the Social Sciences (SPSS.22®). The Kolmogorov-Smirnov test was used to evaluate the distribution of the data, and since the data did not following a normal distribution, proportions and median (minimum-maximum) values were used.
Results: The 53 patients included in the study had singleton pregnancies. The distribution of autoantibodies was as follows: thyroid peroxidase (n=17); antithyroglobulin (n=11); double-stranded DNA (n=4); antinuclear (n=8); anti-smooth muscle (n=1); and anticardiolipin IgG and IgM (n=1). Autoimmune diseases included Hashimoto's thyroiditis (n=23); SLE (n=7); Behcet's disease (n=1); Sjogren's syndrome (n=1); ulcerative colitis (n=1); and anti-phospholipid antibody syndrome (n=1). Ten patients had heterozygous Factor V Leiden thrombophilia; two had homozygous Factor 5 Leiden thrombophilia; and three had the prothrombin 20210A heterozygous mutation. Twenty-eight patients were positive for autoantibodies and hereditary thrombophilia and/or MTHFR polymorphisms.
Conclusions: Evaluation and management of hereditary thrombophilia, MTHFR gene polymorphisms, and/or autoimmune conditions may be beneficial for patients with unexplained infertility.
Keywords: infertility, in vitro fertilization, methylenetetrahydrofolate reductase, autoimmunity.
INTRODUCTION
Infertility is defined as a couple's inability to achieve pregnancy after abstaining from contraceptive methods for 12 months. The prevalence of primary infertility - a term coined to categorize couples unable to achieve their first pregnancy - is approximately 1.9% (Mascarenhas et al ., 2012). The time interval accepted for women aged 35 years or older is six months (Practice Committee of American Society for Reproductive Medicine, 2013).
In the absence of an explainable cause after comprehensive examination, couples are diagnosed with unexplained infertility (UI). Comprehensive examination is expected to reveal the following: 1) regular ovulation, 2) tubal patency, 3) a normal uterine cavity, 4) normal semen analysis results, and 5) an adequate ovarian oocyte reserve (Practice Committee of American Society for Reproductive Medicine, 2013). Expectant management, lifestyle changes, timed intercourse, and intrauterine insemination (IUI) with gonadotropin stimulation or in vitro fertilization (IVF) are different treatment options for UI (Nandi et al ., 2017; Quaas & Dokras, 2008).
IVF has been an effective treatment method for infertile couples performed with high success rates for nearly four decades (Steptoe & Edwards, 1978; Elizur et al ., 2006). It has become the preferred treatment modality for individuals with tubal factor infertility, diminished ovarian reserve, and severe male factor infertility (Rongieres, 2015). However, the role of IVF in patients with UI has not been clearly determined (Rongieres, 2015).
Maternal health disorders (epigenetic, metabolic, immunological conditions, etc.) that affect gametogenesis, fertilization, and implantation may also be linked to UI (Azem et al., 2004; Deroux et al., 2017; Coulam & Jeyendran, 2009; Zhong et al., 2012; Qublan et al., 2006). It has been reported that metabolic pathway disorders including aminoacyl-tRNA biosynthesis, "glycine-serine-threonine" metabolism, "alanine-aspartate-glutamate" metabolism, "valine-leucine-isoleucine" biosynthesis, and methionine metabolism may be linked to impaired gametogenesis and/or unsuccessful implantation (Spiridonov et al., 2005; Ni et al., 2016; Unni et al., 2015). Autoimmune disorders (autoimmune antibody positivity and related diseases) may also be responsible for undesired biological processes such as uterine inflammation, which further lead to impaired endometrial receptivity and placentation (Deroux et al., 2017; Chen et al ., 2017). Thus, methylation disorders and immunological conditions seem to play important roles in the pathophysiology of UI (Azem et al., 2004; Coulam & Jeyendran, 2009).
This study aimed to describe the impact on achieving spontaneous pregnancy of treating patients with at least one failed in-vitro fertilization (IVF) cycle for autoimmune disorders, hereditary thrombophilia, and methylation disorders.
MATERIALS AND METHODS
We evaluated 53 patients with at least one failed IVF cycle for the treatment of primary UI who became pregnant spontaneously and gave birth at our hospital (between January 2007-October 2017) as a consequence of proper management of their medical conditions (autoimmune disorders, hereditary thrombophilia, and MTHFR polymorphisms). The required data were extracted from the Hacettepe University patient database.
All patients with primary UI and at least one failed IVF cycle were included in a special follow-up program and evaluated before conception. The patients were screened for hereditary thrombophilias (factor V Leiden mutation, prothrombin 20210A mutation, protein C/S deficiency), MTHFR polymorphisms, serum vitamin B12/folate/homocysteine levels, autoimmune antibody positivity (antinuclear (ANA), thyroid peroxidase (TPO), antithyroglobulin (TgAb), anti-parietal cell (APA), and antiphospholipid antibodies depending on their clinical findings and family history), and related disease/syndromes at the Hacettepe University, Division of Perinatology. Patients in a quiescent period in terms of immunological and metabolic inflammatory processes were allowed to get pregnant.
All patients were included in a special antenatal care program and had low molecular weight heparin (LMWH = enoxaparin 2000 Anti-Xa IU/0.2 ml), oral prednisone (methylprednisolone 4 mg), and aspirin (acetylsalicylic acid 100 mg) added to their specific treatment protocols as soon as they became pregnant. A special low-methionine diet was prescribed to patients with MTHFR polymorphisms.
Pregnancy follow-up comprised serial laboratory testing and ultrasound examination, aneuploidy screening (combined or triple test), fetal anatomy scanning at the 20th-24th week of gestation, oral glucose challenge test, and non-stress tests weekly (after the 28th week of gestation). All medications were stopped three days before delivery.
The median (minimum-maximum) values of patient age; duration of infertility; number of previous IVF cycles; serum folate, vitamin B12, and homocysteine levels just before conception; gestational week at birth; birth weight; and 5-minute APGAR scores were calculated, as the data did not follow a normal distribution. The proportions of patients with positive tests for autoantibodies, autoimmune diseases, hereditary thrombophilia, and MTHFR polymorphisms were also recorded.
Statistical analyses were performed on the Statistical Package for the Social Sciences (SPSS.22®, IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). The Kolmogorov-Smirnov test was used to assess the distribution of the data, and since the data did not follow a normal distribution, proportions and median (minimum-maximum) values were used.
This study was approved by the Ethics Committe at Hacettepe University Et (GO 18/158).
RESULTS
The 53 singleton pregnancies resulted in live births. There were no ectopic pregnancies, miscarriages, or stillbirths. There were only three spontaneous late preterm births (5.6%) (at 34, 35, and 35 weeks of gestation). Preeclampsia, eclampsia, and placental abruption were not observed in any of the patients.
Table 1 shows the median and minimum-maximum values for maternal age; number of previous IVF cycles; duration of infertility; gestational week at birth; birth weight; 5-minute APGAR score; and serum folate, vitamin B12, and homocysteine levels.
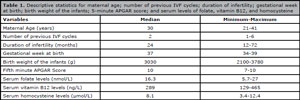
Table 1. Descriptive statistics for maternal age; number of previous IVF cycles; duration of infertility; gestational week at birth; birth weight of the infants; 5-minute APGAR score; and serum levels of folate, vitamin B12, and homocysteine
Table 2 shows the proportions for autoantibodies. Table 3 shows the proportions for hereditary thrombophilias, MTHFR polymorphisms, and autoantibody positivity together with thrombophilias
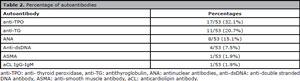
Table 2. Percentage of autoantibodies
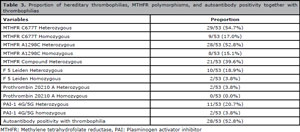
Table 3. Proportion of hereditary thrombophilias, MTHFR polymorphisms, and autoantibody positivity together with thrombophilias
Twenty-three patients (43.4%) had Hashimoto's thyroiditis; seven (13.2%) had SLE; one (1.9%) had Behcet's Disease; one had Sjogren's syndrome; one (1.9%) had ulcerative colitis; and one (1.9%) had anti-phospholipid antibody syndrome.
The 53 patients had at least one hereditary thrombophilia and/or MTHFR polymorphism. Autoantibody positivity was seen in 28 patients (52.8%) combined with hereditary thrombophilia and/or MTHFR polymorphisms.
DISCUSSION
Although IVF is the most successful treatment method for UI, its overall live birth rate is approximately 40%, depending on maternal age and the number of transferred embryos (Elizur et al., 2006). Infertility is a multifactorial condition that affects couples in medical, psychological, sociological, and economic aspects (Péloquin et al., 2018). Some identifiable risk factors are genetic abnormalities, ovulatory disorders, tubal damage, uterine or peritoneal problems, and male factors (Ray et al., 2012). On the other hand, nearly 30% of couples have no determined etiology (Ray et al., 2012).
The complexity of the situation emphasizes the need for further investigation. Hyperhomocysteinemia, MTHFR gene polymorphisms, variations in folate pathway genes, vitamin B-complex deficiencies, hereditary thrombophilias, and autoimmune antibody production are some factors that contribute to the etiology of UI (Deroux et al., 2017; Altmäe et al., 2010; Das et al., 2015; Hou et al., 2016; Enciso et al., 2016).
Thrombophilia can cause infertility as it impairs oocyte quality, increases hypoxic damage, and diminishes vascularization (Qublan et al., 2006). Properly vascularized and oxygenated follicles lead to higher rates of implantation (Qublan et al., 2006; Chui et al., 1997). It has been shown that during IVF the mean follicular diameter, oocyte retrieval rate, number of mature oocytes, and fertilization rates are higher in highly vascularized follicles (Qublan et al., 2006; Bhal et al., 1999). Implantation, placentation, angiogenesis, and vascular remodeling require an appropriate balance between coagulation and fibrinolysis, although thrombosis in the intervillous space and placental vessels may cause placental insufficiency (Qublan et al ., 2006). On the other hand, heparin has a role in trophoblast differentiation and invasion (Lodigiani et al ., 2017; Nelson & Greer, 2008). More specifically, low-molecular-weight heparin (LMWH) affects matrix metalloproteinases (MMP), tissue inhibitors, cadherin-E, heparin-binding epidermal growth factor (HBEGF), and insulin-like growth factor (IGF) (Lodigiani et al., 2017; Nelson & Greer, 2008; Di Simone et al., 2007; Erden et al., 2006; Das et al., 1994; Lacey et al., 2002). LMWH also has a positive effect on IVF outcomes (Lodigiani et al., 2017). These findings support our results, which indicated that appropriate management of thrombophilia and proper therapy with heparin play a significant role in the treatment of UI.
Methionine is an essential amino acid in nucleic acid synthesis and homocysteine is a metabolite resulting from its metabolism (Das et al., 2015). High levels of homocysteine may arise from deficiency of certain vitamins (folic acid, vitamin B6, etc.) and/or MTHFR gene polymorphisms (Das et al., 2015). Hyperhomocysteinemia causes many adverse pregnancy outcomes, including pregnancy loss, neural tube defects, chromosomal aneuploidies, fetal cardiac defects, preeclampsia, placental abruption, and intrauterine growth restriction (IUGR) (Das et al., 2015; Ray & Laskin, 1999; Botto & Yang, 2000). Hyperhomocysteinemia has also been associated with impaired follicular development, oxidative damage to oocytes, improper vascularization of the chorionic villi, and implantation failure (Das et al., 2015; Jerzak et al ., 2003). Therefore, deficiencies in folate and/or B-complex vitamins lead to the accumulation of homocysteine and may cause UI (Altmäe et al ., 2010). Some of the hypothesized mechanisms include impaired cell division, increased production rates of inflammatory cytokines, impaired nitric oxide metabolism, increased oxidative stress, increased rates of apoptosis, and impaired methylation reactions. All these factors combined affect oocyte development and embryo implantation and reduce endometrial receptivity (Altmäe et al., 2010). Thus, supplementation with folate and B-complex vitamins before conception decreases homocysteine levels in the follicular fluid, which leads to decreased rates of infertility and lower rates of miscarriage (Altmäe et al., 2010; Chavarro et al., 2008). Heterozygous mutations of the gene coding the MTHFR enzyme decrease enzyme activity by 35%, while homozygous mutations decrease activity by 70%, thus causing impaired folate metabolism and accumulation of homocysteine (Frosst et al., 1995). Several studies in the literature have described the negative effects of high homocysteine levels in patients with infertility and/or polycystic ovary syndrome (PCOS) (D'Uva et al., 2007; Bibi et al ., 2010; Schachter et al ., 2003). These findings are consistent with our results. Appropriate management of decreased serum homocysteine levels and increasing serum folate and vitamin B levels are essential for the treatment of UI.
Autoimmune factors seem to play a pivotal role in infertility (Chen et al., 2017). The prevalence of antiphospholipid antibodies (aPL), ANA, and antithyroid antibodies was found to be particularly higher in women with UI (Chen et al., 2017). Implantation is a process that necessitates immunologic tolerance and requires cross-talk between the embryo and the maternal immune system (Kushnir et al., 2016). Impaired implantation and high pregnancy loss rates in women with autoimmune antibodies may be caused by injury to the syncytiotrophoblasts, endovascular trophoblasts covering the tip of the spiral arteries, endothelial cells of the spiral veins, superficial/glandular epithelial cells of the decidua, autoantibody inflammatory processes, and entrance of cell degradants from these tissues into the maternal circulation. These biological events result in impaired implantation and disturbed fetal perfusion (Beksaç et al., 2017). In addition to these, ovulation, implantation, and onset of labor are thought to be associated with inflammation (Kushnir et al., 2016; Weiss et al., 2009). Although exact screening and management protocols for infertile patients positive for autoimmune antibodies have not been established, it seems reasonable to devise a patient-centered, individualized approach for these patients. Low-dose methylprednisolone (4 mg, once a day), low-dose acetylsalicylic acid (100 mg once a day), and low-dose LMWH (20 mg/0.2 ml enoxaparin sodium administered intramuscularly once a day) were the main components of treatment, as it has been shown that heparin and heparin-related derivatives have an anti-inflammatory effect (Young, 2008).
Although IVF is a revolutionary treatment for infertile couples, use without appropriate indication may increase both costs and procedure-related complications (Ben-Ami et al., 2017). Ovarian hyperstimulation syndrome, multiple pregnancy, preterm labor, preeclampsia, and increased rates of chromosomal/structural abnormalities are some of the complications related with the IVF procedure (Ben-Ami et al., 2017; Xu et al., 2015).
The 53 patients had at least one underlying condition (hereditary thrombophilia, MTHFR gene polymorphism, or autoantibody positivity). After the introduction of appropriate management protocols, all patients delivered healthy babies. Preeclampsia, eclampsia, and placental abruption were not observed in any of the patients. There were only three spontaneous late preterm deliveries (5.6%) (at 34, 35 and 35 weeks of pregnancy, respectively).
The limitations of this study are the small number of patients, its retrospective design, and the fact that it reflects the experience of a single center. Furthermore, this is a descriptive assessment of a very specific group of patients who gave birth at our institution without the aid of assisted reproductive technology and who had a history of failed IVF cycles for UI. This study was not designed to investigate the success rate of our management protocol, but to stress the importance of knowing the etiological factors behind UI.
In conclusion, infertility is a field with plenty to discover. Underlying maternal conditions may cause conception failure. Evaluation and management of hereditary thrombophilias, MTHFR gene polymorphisms, and/or autoimmune conditions may be beneficial for primary infertility patients with at least one failed IVF cycle.
Funding/Support Statement
No funding was used fort his study.
ACKNOWLEDGMENTS
The authors would like to thank the medical staff of our institution for working tirelessly to provide their patients with optimal healthcare.
REFERENCES
Altmäe S, Stavreus-Evers A, Ruiz JR, Laanpere M, Syvänen T, Yngve A, Salumets A, Nilsson TK. Variations in folate pathway genes are associated with unexplained female infertility. Fertil Steril. 2010;94:130-7.
Medline Crossref
Azem F, Many A, Yovel I, Amit A, Lessing JB, Kupferminc MJ. Increased rates of thrombophilia in women with repeated IVF failures. Hum Reprod. 2004;19:368-70.
Medline Crossref
Beksaç K, Örgül G, Çagan M, Karaağaoğlu E, Arslan S, Beksaç MS. Retrospective evaluation of pregnant women with celiac disease. J Turk Ger Gynecol Assoc. 2017;18:56-9.
Medline Crossref
Bhal PS, Pugh ND, Chui DK, Gregory L, Walker SM, Shaw RW. The use of transvaginal power Doppler ultrasonography to evaluate the relationship between perifollicular vascularity and outcome in in-vitro fertilization treatment cycles. Hum Reprod. 1999;14:939-45.
Medline Crossref
Botto LD, Yang Q. 5,10-Methylenetetrahydrofolate reductase gene variants and congenital anomalies: a HuGE review. Am J Epidemiol. 2000;151:862-77.
Medline Crossref
Chavarro JE, Rich-Edwards JW, Rosner BA, Willett WC. Use of multivitamins, intake of B vitamins, and risk of ovulatory infertility. Fertil Steril. 2008;89:668-76.
Medline Crossref
Chen X, Mo ML, Huang CY, Diao LH, Li GG, Li YY, Lerner A, Shoenfeld Y, Zeng Y. Association of serum autoantibodies with pregnancy outcome of patients undergoing first IVF/ICSI treatment: A prospective cohort study. J Reprod Immunol. 2017;122:14-20.
Medline Crossref
Chui DK, Pugh ND, Walker SM, Gregory L, Shaw RW. Follicular vascularity--the predictive value of transvaginal power Doppler ultrasonography in an in-vitro fertilization programme: a preliminary study. Hum Reprod. 1997;12:191-6.
Medline Crossref
Coulam CB, Jeyendran RS. Thrombophilic gene polymorphisms are risk factors for unexplained infertility. Fertil Steril. 2009;91:1516-7.
Medline Crossref
Das SK, Wang XN, Paria BC, Damm D, Abraham JA, Klagsbrun M, Andrews GK, Dey SK. Heparin-binding EGF-like growth factor gene is induced in the mouse uterus temporally by the blastocyst solely at the site of its apposition: a possible ligand for interaction with blastocyst EGF-receptor in implantation. Development. 1994;120:1071-83.
Medline
Das V, Misra D, Agrawal S, Agrawal A, Pandey A. Hyperhomocysteinemia and MTHFR gene 677 C>T polymorphism: questionable role in female infertility. Int J Reprod Contracept Obstet Gynecol. 2015;4:683-9.
Crossref
Deroux A, Dumestre-Perard C, Dunand-Faure C, Bouillet L, Hoffmann P. Female infertility and serum auto-antibodies: a systematic review. Clin Rev Allergy Immunol. 2017;53:78-86.
Medline Crossref
Di Simone N, Di Nicuolo F, Sanguinetti M, Ferrazzani S, D'Alessio MC, Castellani R, Bompiani A, Caruso A. Low-molecular weight heparin induces in vitro trophoblast invasiveness: role of matrix metalloproteinases and tissue inhibitors. Placenta. 2007;28:298-304.
Medline Crossref
D'Uva M, Di Micco P, Strina I, Alviggi C, Iannuzzo M, Ranieri A, Mollo A, De Placido G. Hyperhomocysteinemia in women with unexplained sterility or recurrent early pregnancy loss from Southern Italy: a preliminary report. Thromb J. 2007;5:10.
Medline Crossref
Elizur SE, Lerner-Geva L, Levron J, Shulman A, Bider D, Dor J. Cumulative live birth rate following in vitro fertilization: study of 5,310 cycles. Gynecol Endocrinol. 2006;22:25-30.
Medline Crossref
Enciso M, Sarasa J, Xanthopoulou L, Bristow S, Bowles M, Fragouli E, Delhanty J, Wells D. Polymorphisms in the MTHFR gene influence embryo viability and the incidence of aneuploidy. Hum Genet. 2016;135:555-68.
Medline Crossref
Erden O, Imir A, Guvenal T, Muslehiddinoglu A, Arici S, Cetin M, Cetin A. Investigation of the effects of heparin and low molecular weight heparin on E-cadherin and laminin expression in rat pregnancy by immunohistochemistry. Hum Reprod. 2006;21:3014-8.
Medline Crossref
Frosst P, Blom HJ, Milos R, Goyette P, Sheppard CA, Matthews RG, Boers GJ, den Heijer M, Kluijtmans LA, van den Heuve LP, Rozen R. A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet. 1995;10:111-3.
Medline Crossref
Hou N, Chen S, Chen F, Jiang M, Zhang J, Yang Y, Zhu B, Bai X, Hu Y, Huang H, Xu C. Association between premature ovarian failure, polymorphisms in MTHFR and MTRR genes and serum homocysteine concentration. Reprod Biomed Online. 2016;32:407-13.
Medline Crossref
Kushnir VA, Solouki S, Sarig‐Meth T, Vega MG, Albertini DF, Darmon SK, Deligdisch L, Barad DH, Gleicher N. Systemic inflammation and autoimmunity in women with chronic endometritis. Am J Reprod Immunol. 2016;75:672-7.
Medline Crossref
Lacey H, Haigh T, Westwood M, Aplin JD. Mesenchymally-derived insulin-like growth factor 1 provides a paracrine stimulus for trophoblast migration. BMC Dev Biol. 2002;2:5.
Medline Crossref
Lodigiani C, Dentali F, Banfi E, Ferrazzi P, Librè L, Quaglia I, Cafaro L , Morenghi E, Pacetti V, Zannoni E, Baggiani AM, Levi-Setti PE. The effect of parnaparin sodium on in vitro fertilization outcome: A prospective randomized controlled trial. Thromb Res. 2017;159:116-21.
Medline Crossref
Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLoS Med. 2012;9:e1001356.
Medline Crossref
Nandi A, Bhide P, Hooper R, Gudi A, Shah A, Khan K, Homburg R. Intrauterine insemination with gonadotropin stimulation or in vitro fertilization for the treatment of unexplained subfertility: a randomized controlled trial. Fertil Steril. 2017;107:1329-35.e2.
Medline Crossref
Nelson SM, Greer IA. The potential role of heparin in assisted conception. Hum Reprod Update. 2008;14:623-45.
Medline Crossref
Ni H, Lu L, Deng J, Fan W, Li T, Yao J. Effects of Glutamate and Aspartate on Serum Antioxidative Enzyme, Sex Hormones, and Genital Inflammation in Boars Challenged with Hydrogen Peroxide. Mediators Inflamm. 2016;2016:4394695.
Medline Crossref
Péloquin K, Brassard A, Arpin V, Sabourin S, Wright J. Whose fault is it? Blame predicting psychological adjustment and couple satisfaction in couples seeking fertility treatment. J Psychosom Obstet Gynaecol. 2018;39:64-72.
Medline Crossref
Practice Committee of American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2013;99:63.
Medline Crossref
Quaas A, Dokras A. Diagnosis and treatment of unexplained infertility. Rev Obstet Gynecol. 2008;1:69-76.
Medline
Qublan HS, Eid SS, Ababneh HA, Amarin ZO, Smadi AZ, Al-Khafaji FF, Khader YS. Acquired and inherited thrombophilia: implication in recurrent IVF and embryo transfer failure. Hum Reprod. 2006;21:2694-8.
Medline Crossref
Ray JG, Laskin CA. Folic acid and homocyst(e)ine metabolic defects and the risk of placental abruption, pre-eclampsia and spontaneous pregnancy loss: A systematic review. Placenta. 1999;20:519-29.
Medline Crossref
Ray A, Shah A, Gudi A, Homburg R. Unexplained infertility: an update and review of practice. Reprod Biomed Online. 2012;24:591-602.
Medline Crossref
Schachter M, Raziel A, Friedler S, Strassburger D, Bern O, Ron‐El R. Insulin resistance in patients with polycystic ovary syndrome is associated with elevated plasma homocysteine. Hum Reprod. 2003;18:721-7.
Medline Crossref
Spiridonov NA, Wong L, Zerfas PM, Starost MF, Pack SD, Paweletz CP, Johnson GR. Identification and Characterization of SSTK, a serine/threonine protein kinase essential for male fertility. Mol Cell Biol. 2005;25:4250-61.
Medline Crossref
Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 1978;2:366.
Medline
Unni SN, Lakshman LR, Vaidyanathan K, Subhakumari KN, Menon NL. Alterations in the levels of plasma amino acids in polycystic ovary syndrome--A pilot study. Indian J Med Res. 2015;142:549-54.
Medline Crossref
Weiss G, Goldsmith LT, Taylor RN, Bellet D, Taylor HS. Inflammation in reproductive disorders. Reprod Sci. 2009;16:216-29.
Medline Crossref
Xu XY, Yang JH, Ma XM, Liu AL, Liu K, He S, Mi HY, Li L. Neonatal complications and birth defects in infants conceived by in vitro fertilization. Zhongguo Dang Dai Er Ke Za Zhi. 2015;17:350-5.
Medline Crossref
Young E. The anti-inflammatory effects of heparin and related compounds. Thrombosis Res. 2008;122:743-52.
Medline Crossref
Zhong YP, Ying Y, Wu HT, Zhou CQ, Xu YW, Wang Q, Li J, Shen XT, Li J. Relationship between antithyroid antibody and pregnancy outcome following in vitro fertilization and embryo transfer. Int J Med Sci. 2012;9:121-5.
Medline Crossref