JBRA Assist. Reprod 2006;10(2):21-24
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2006.10.2.05
Comparison of 150 IU and 225 IU of Follitropin-β in a Fixed-dose Regimen for Ovarian Stimulation Using a Depot Formulation of GnRH Agonist: a prospective randomized clinical trial
Comparação Entre 150 UI e 225 UI de Folitropina-β em Regime de Dose Fixa para Estimulação Ovariana com o Uso de Formulação Depot de Agonista do GnRH: Estudo Prospectivo e Randomizado
Centro de Referência da Saúde da Mulher, Hospital Pérola Byington, São Paulo
ABSTRACT
This prospective and randomized study included 76 normoovulatory women undergoing assisted reproductive technology cycles using the long protocol of GnRH agonist who received either 150 IU (group A, n=40) or 200 IU (group B, n=36) of recombinant FSH (follitropin-β) per day in a fixed-dose regimen. Four outcome measures including percentage of mature oocytes collected, fertilization rate, pregnancy rate and total dose of follitropin-β administered were compared between the groups. Percentage of mature oocytes retrieved (91% in group A versus 87.1% in group B), fertilization rate (69% in group A versus 74% in group B) and pregnancy rate per transfer (25.0% in group A versus 26.6% in group B), were not statistically different in both groups. The mean dose of recombinant FSH administered was lower in group A (1,620 ± 215 IU in group A versus 2,078 ± 275 in group B). It is concluded that the dose of 150 IU of follitropin-β is more cost-effective and may be the dose of choice to be employed for ovarian stimulation with a fixed-dose regimen in normo-ovulatory women with age less than 35 years.
Palavras-chave: estimulação ovariana, protocolo de estimulação com dose fixa, FSH recombinante, folitropina-b, agonista do GnRH.
RESUMO
Foram estudadas, prospectivamente, 76 mulheres normo-ovulatórias submetidas a procedimentos de reprodução assistida com esquema de estimulação ovariana empregando o protocolo longo com agonista do GnRH na forma depot. As pacientes foram randomizadas para receber 150 UI (grupo A, n=40) ou 200 UI (grupo B, n=36) de FSH recombinante (folitropina-β) em dose fixa diária. Comparou-se, entre os dois grupos, a porcentagem de oócitos maduros coletados, as taxas de fertilização e gravidez e a dose total de folitropina-β administrada. Não houve diferença estatisticamente significante entre os grupos na porcentagem de oócitos maduros coletados (91% no grupo A versus 87,1% no grupo B), na taxa de fertilização (69% no grupo A versus 74% no grupo B) e na taxa de gravidez por transferência (25,0% no grupo A versus 26,6% no grupo B). A dose média de FSH administrada foi menor no grupo A (1.620 ± 215 UI no grupo A versus 2.078 ± 275 no grupo B). Concluiu-se que o emorego de 150 UI de folitropina-β apresenta um melhor custo/benefício e pode ser considerada a dose de escolha para a estimulação ovariana em regime de dose fixa em mulheres normo-ovulatórias com menos de 35 anos.
Key words: ovarian stimulation, fixed-dose stimulation protocol, recombinant FSH, follitropin-β, GnRH agonist
INTRODUCTION
Ovarian stimulation is a standard procedure in assisted reproductive technologies (ART), in order to stimulate the growth of several follicles and consequently obtain as many good quality oocytes as possible. Over the last four decades, urinary gonadotropins have been employed for this purpose, and urinary follicle-stimulating hormone (u-FSH) of different purity has been developed. In the last decade, FSH with a much higher purity has become available by using recombinant DNA technique (Out et al., 1995; Shoham and Insler, 1996). The two recombinant FSH (r-FSH) preparations currently available for clinical use are follitropin-a, marketed as Gonal-F® by Ares- Serono, and follitropin-ß, marketed as Puregon® by NV Organon. Although there still is no consensus regarding the superiority of recombinant over urinary gonadotropins, many investigators consider that r-FSH has advantages in comparison with the older urinary preparations, and provides better cost-effectiveness in ART treatment (Bergh, 1999; Daya et al., 2002; Silverberg et al., 2002; Goldfarb and Desai, 2003; Cheon et al., 2004; Palagiano et al., 2004; Bassett and Driebergen, 2005).
Protocols for ovarian stimulation are usually performed with a starting dose of urinary or recombinant gonadotropins, and after a period of 5-7 days of stimulation, the daily gonadotropin dose is adjusted according to ovarian response. Nevertheless, regimens of ovarian-controlled stimulation using fixed daily doses of gonadotropins can be an interesting option for the treatment of infertile couples undergoing ART procedures. The fixed-dose regimens are employed to simplify the procedures of ovarian stimulation, which is an important goal to achieve, reducing costs and increasing treatment compliance. Furthermore, it remains to be determined whether dose changes during controlled ovarian stimulation are useful, because there is evidence that follicular response to alterations in the FSH dose is not evident before at least 4 days (Out et al., 1999). Another way of simplifying the ART treatment is to employ the long-term protocol with a depot formulation of GnRH agonist, which induces pituitary desensitization through a single administration of the analogue in the mid-luteal phase of the menstrual cycle preceding the ART procedure. Even if the use of depot formulations is thought to induce a too high pituitary suppression, it does not seem to be deleterious to the ART cycle outcome when compared with short formulations in normally responding women (Albuquerque et al., 2003; Dal Prato et al., 2004). This study aims at comparing 150 IU and 200 IU of follitropin-ß in a fixed-dose regimen, employing the long protocol of pituitary down-regulation with a depot formulation of GnRH agonist, in normo-ovulatory women undergoing in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI) cycles.
MATERIALS AND METHODS
We studied 76 normo-ovulatory women < 35 years old, undergoing ART cycles at the Unit of Assisted Reproduction of the Centro de Referência da Saúde da Mulher, Hospital Pérola Byington, in São Paulo. All patients had indications for treatment with IVF or ICSI cycles. The inclusion criteria used were as follows: age < 35 years old, normal menstrual cycles (range of 24-35 days), body mass index between 19 and 29 kg⁄m2, and FSH < 10 mIU/mL. The exclusion criteria were as follows: age < 18 and > 35 years old, endocrine abnormalities, previous ART cycle with poor response to ovarian stimulation, and systemic chronic disease. After pituitary suppression with a single intramuscular administration of a GnRH agonist (Lupron® 3.75, Abbott, Brazil), patients were randomized into groups A and B. In group A (n=40), ovarian stimulation was performed with a fixed daily dose of 150 IU of follitropin-ß (Puregon®, Organon, Brazil). In group B (n=36), ovarian stimulation was performed with a fixed daily dose of 200 IU of follitropin-ß. In both groups, the fixed dose was maintained until hCG administration. When at least three follicles = 17 mm had developed, ovulation was triggered with 10,000 IU of hCG (Profasi®, Serono, Brazil) or 250 µg of recombinant hCG (Ovidrel®, Serono, Brazil). Cycle monitoring was carried out using only ultrasound findings. Cycles were cancelled due to risk for OHSS when a total of >20 follicles with mean diameter = 5 mm were identified on ultrasound scan at any stage of ovarian stimulation. If there was an insufficient follicular growth (<3 follicles developed in response to ovarian stimulation), cycles were cancelled due to poor response. Follicular aspiration was scheduled 35-36 hours after the hCG administration. The luteal phase was supported daily with 90mg of intravaginal progesterone gel (Crinone®, Serono, Brazil). The cancellation rates, the number of mature oocytes retrieved, the fertilization rate and the pregnancy rate determined by fetal heart, and the total dose of recombinant FSH administered, were evaluated in the two groups. Chi square and student’s t test were utilized when appropriate, and P < 0.05 was considered significant.
RESULTS
Both treatment groups were comparable in demographic and infertility characteristics. Results are shown in Table 1. In group A, 1 cycle (2.5%) was cancelled because of risk for ovarian hyperstimulation syndrome (OHSS) determined by ultrasonography parameters. In group B, 3 cycles (8%) were cancelled, 2 because of risk for OHSS, and 1 because of poor response to ovarian stimulation. The cancellation rates were not statistically different in either group (P > 0.05). The number of oocytes retrieved was similar in groups A and B. In group A, 225 oocytes were retrieved (mean: 7.03 per cycle) and in group B, 233 oocytes were collected (mean: 7.06 per cycle). Percentage of mature oocytes retrieved (91% in group A versus 87.1% in group B), fertilization rate (69% in group A versus 74% in group B), and pregnancy rate per transfer (25.6% in group A versus 27.3% in group B) were not statistically different in either group (P > 0.05). The mean dose of recombinant FSH administered was significantly lower in group A (1,620 ± 215 IU in group A versus 2,078 ± 275 in group B; P < 0.05). The outcome of ART cycles are summarized in Table 2.
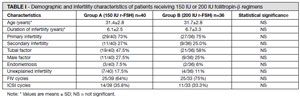
TABLE I. Demographic and infertility characteristics of patients receiving 150 IU or 200 IU follitropin-β regimens
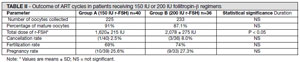
TABLE II. Outcome of ART cycles in patients receiving 150 IU or 200 IU follitropin-β regimens
DISCUSSION
The optimal dose of r-FSH needed for ovarian stimulation for ART remains to be determined. Most protocols commence with a daily administration of 150 - 225 IU of r-FSH, and adjust the dose according to ovarian response, by employing step up or step down regimens (Cohen, 2003). There is evidence that a starting dose of 150 IU of r-FSH may be the best approach to normally responding patients. Harrison et al. (2001), comparing starting doses of 150 and 200 IU of r-FSH in IVF and ICSI cycles, reported that there is little advantage in using the higher dose. Out et al. (2004) reported that increasing the starting dose from 150 to 200 IU of r-FSH, slightly more oocytes can be retrieved in GnRH antagonist protocols for assisted reproduction, without the achievement of a higher number of good quality embryos. Recently, Tan et al. (2005) registered that patients undergoing ART cycles have similar outcomes whether r-FSH is commenced in a dose of 100 IU or of 200 IU for the first 4 days of stimulation. Thus, in flexible protocols, it is possible to recommend the starting dose of 100-150 IU of r-FSH, at least in normally responding women. Currently, in order to simplify ART treatment, many groups perform controlled ovarian stimulation with a fixed-dose regimen of r-FSH, utilizing either GnRH agonists or antagonists (Eldar-Geva et al., 2000; Balasch et al., 2003; Hohmann et al., 2003; Cheung et al., 2005). The use of a fixed-dose regimen may have some advantages over flexible protocols, such as making the treatment simpler and allowing the possibility of a minimal monitoring protocol. Hurst et al. (2003), employing a fixed-dose stimulation regimen in normoovulatory women, performed minimally monitored cycles, limited to a single ultrasound performed 8 or 9 days after stimulation. These authors achieved high pregnancy and implantation rates (51% and 23%, respectively) and concluded that the reduction of time, commitment, and cost led to a high patient acceptance of this approach. In our investigation, cycle monitoring was carried out only with ultrasound scans, and hormonal dosages were not performed, with the purpose of simplifying and reducing the costs of the ART procedure.
Many investigators compared different doses of gonadotropins for ovarian stimulation, using fixed-dose regimens. Out et al. (1999) employed 100 and 200 IU of r-FSH in a fixed-dose regimen and concluded that compared to 200 IU, the use of a 100 IU fixed-dose is less efficacious in terms of the number of oocytes retrieved and is associated with more cycle cancellations. The same group (Out et al., 2000), compared fixed doses of 150 and 250 IU of r-FSH and concluded that in women between 30 and 39 years of age, the decline in number of oocytes retrieved in older women cannot be overcome by increasing the fixed dose of r-FSH. Similarly, the Latin-American Puregon IVF Study Group (2001) compared two different fixed daily doses of follitropin-ß for ovarian stimulation and concluded that an increase from a 150 IU to a 250 IU daily dose of recombinant FSH in women between 30 and 39 years of age has limited value in terms of increasing ovarian response. Hoomans and Mulder (2002) reported that the use of a 100 IU fixed-dose is less effective in terms of the number of oocytes retrieved and the higher cancellation rate, but more efficient as indicated by a lower total recombinant FSH dose needed. Ng et al. (2000) compared protocols with fixed doses of 100 and 200 IU of r-FSH daily in Chinese normo-ovulatory women, and concluded that the use of 100 IU daily results in the retrieval of half the number of oocytes compared to the dosage of 200 IU daily. Yong et al. (2003) comparing 150 IU and 225 IU of r-FSH in a fixed-dose regimen concluded that 225 IU is more effective in younger women, but requires a higher total dose of r-FSH. These authors did not observe any benefits of 225 IU in comparison to 150 IU in older women. Pruksananonda et al. (2004) observed that a fixed daily dose of 200 IU of r-FSH compared to a fixed daily dose of 100 IU is more effective in terms of follicles > 17 mm development and the number of oocytes retrieved along with a lower cancellation rate. Other investigations analyzed the outcomes of ART with a fixed dose of gonadotropins, comparing u-FSH and r-FSH. Hoomans et al. (1999) reported that treatment outcome of a fixed daily dose of 150 IU r-FSH is comparable to a fixed daily dose of 225 IU highly purified u-FSH, with a significantly lower total dose needed in the r-FSH group.
In our randomized clinical trial, 76 normo-ovulatory women < 35 years old received either 150 or 200 IU of follitropin-ß in a fixeddose regimen. The primary outcome measurements were the number of mature oocytes collected and the total dose of r-FSH administered, and secondary parameters included cancellation, fertilization, and pregnancy rates. Considering all 76 patients, we had only one cycle (1.3%) cancelled due to poor ovarian response (group B). This fact is most likely due to the age (<35 years) and ovulatory characteristics (normal menstrual cycles, FSH < 10 mIU/ mL) of the patients. One cycle in group A and 2 cycles in group B, were cancelled due to risk for OHSS determined by echographic parameters. We did not perform estradiol measurements in order to reduce the costs of treatment, and we did not observe any case of moderate/severe OHSS in the 72 women that received hCG injection The results of our investigation did not show a doseresponse relationship between r-FSH and the number of oocytes retrieved. We observed that similar numbers of oocytes were obtained in both groups and there were no significant differences in the percentage of mature oocytes collected. Nevertheless, the total dose of r-FSH was significantly lower in the group of 150 IU. This fact grants a higher cost-effectiveness to this regimen, also because fertilization and pregnancy rates were not different between the two protocols. In summary, our data showed that the fixed dose of 150 IU of recombinant FSH was as efficient as 200 IU in ART cycles, with the same outcomes regarding number of oocytes collected and pregnancy rates, and with a significant lower total dose used in the 150 IU group. This being so, the dose of 150 IU of r-FSH is more cost-effective compared to the dose of 200 IU. In conclusion, the regimen of a fixed dose of 150 IU of r-FSH administered daily, associated to the pituitary desensitization with a depot GnRH agonist administered in the mid-luteal phase of the preceding cycle is an efficient protocol for ovarian stimulation, and may be indicated for normo-ovulatory young women, due to its simplicity and cost-effectiveness.
4. Bergh C. - Recombinant follicle stimulating hormone. Hum. Reprod. 14: 1418-1420, 1999.