JBRA Assist. Reprod. 2011;15(4):15-20
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2011.15.4.02
Predictive Factors of Metabolic Syndrome in Adults and Adolescents with Polycystic Ovary Syndrome
Fatores Preditivos de Síndrome Metabólica em Adultas e Adolescentes com Síndrome dos Ovários Policísticos
Department of Obstetrics and Gynaecology, Medical School of Ribeirão Preto, University of São Paulo, Brazil
Financial support from the National Council of Research and Technology Development (CNPq), process no. 136404/2009-0
ABSTRACT
Objectives: Compare clinical and metabolic parameters, as well as predictors of metabolic syndrome (MS), in adolescent and adult women with polycystic ovary syndrome (PCOS).
Methods: A Cross-sectional study was conduced in Faculty of Medicine of Ribeirão Preto, University of São Paulo. A total of 147 women with PCOS were divided into 2 groups: 42 adolescents and 105 adults. Anthropometric measurements, blood samples and pelvic ultrasound exams were made to assessment of the prevalence of MS and its components. Furthermore, the predictors of MS in women with PCOS were evaluated by multivariate analysis.
Results: The prevalence of increased diastolic blood pressure and changes in the lipid panel was greater in adult women than in adolescents (p<0.02). The prevalence of MS was greater in adult women than in adolescents (49.5% vs. 23.8%, p=0.01). In adult women, insulin levels and body mass index (BMI) were independent predictors of MS incidence (p<0.01), but in adolescents, only BMI was found to be an independent predictor of MS (p<0.03).
Conclusions: The insulin levels and BMI were independent predictors of MS in the adult women with PCOS, however, for adolescents, only the BMI was independent predicted of MS, emphasizing the need to monitor these patients from adolescence to prevent metabolic complications.The study was approved by the ethics committee through the process HCRP 3505/2009.
Keywords: Polycystic ovary syndrome, adolescent, insulin, obesity, metabolic syndrome
RESUMO
Objetivo: Comparar os parâmetros clínicos e metabólicos, assim como os preditores de Síndrome Metabólica (SM), em mulheres adolescentes e adultas com Síndrome dos Ovários Policísticos (SOP).
Métodos: Um estudo transversal foi conduzido na Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo. Um total de 147 mulheres com SOP foram divididas em dois grupos: 42 adolescentes e 105 adultas. As medidas antropométricas, amostras de sangue e exames de ultra-sonografia pélvica foram feitas para avaliação da prevalência de SM e seus componentes. Além disso, os preditores de SM em mulheres com SOP foram avaliados por análise multivariada.
Resultados: A prevalência do aumento da pressão arterial diastólica e alterações no perfil lipídico foi maior em mulheres adultas do que em adolescentes (p <0,02). A prevalência da SM foi maior em mulheres adultas do que em adolescentes (49,5% versus 23,8%, p = 0,01). Em mulheres adultas, os níveis de insulina e o índice de massa corporal (IMC) foram preditores independentes da incidência de SM (p <0,01), mas em adolescentes, apenas o IMC foi considerado um preditor independente de SM (p <0,03).
Conclusões: Os níveis de insulina e o IMC foram preditores independentes de SM nas mulheres adultas com SOP, no entanto, para as adolescentes, apenas o IMC foi preditor independente de SM, enfatizando a necessidade de monitorar essas pacientes desde a adolescência para prevenir complicações metabólicas.O estudo foi aprovado pelo Comitê de Ética através do processo HCRP 3505/2009.
Palavras-chave: síndrome dos ovários policísticos, adolescentes, insulina, obesidade, síndrome metabólica
INTRODUCTION
Polycystic ovary syndrome (PCOS) is a reproductive endocrine disorder that has an onset of symptoms during adolescence and affects approximately 5 to 10% of the female population of reproductive age (Rosenfield, 2007; Aribi, 2008). These women may present with clinical signs such as infertility, irregular menses or hyperandrogenism (based on clinical and/or laboratory evidence), generally accompanied by weight gain; overweight or obesity occurs in approximately half of PCOS cases (Gambineri et al., 2002).
Other metabolic disorders may be associated with PCOS, such as hyperinsulinemia, insulin resistance (IR), metabolic syndrome (MS), early-onset type 2 diabetes mellitus (DM2), dyslipidemia and increased risk of cardiovascular disease (Ehrmann et al., 1999).
The discovery of a high prevalence of IR in women affected by PCOS, regardless of weight, has resulted in a greater appreciation of IR in the pathophysiology of this condition (Goodarzi et al., 2005). IR is detected in 50 to 90% of women with PCOS, and the prevalence is higher in obese patients (Carmina & Lobo, 2004). Studies have shown early changes in the sensitivity and secretion of insulin over a lifetime course of PCOS, indicating that similarly to adult women, adolescents with PCOS, whether thin or obese, have a higher risk of glucose intolerance and DM2 (Silfen et al., 2003).
PCOS may be hereditary, and the interaction of genetic and environmental factors appears to play a fundamental role in its onset. Prepubertal daughters of patients with PCOS have been reported to have an increased incidence of polycystic ovaries, diagnosed by ultrasonography, without changes in circulating androgen or luteinizing hormone (LH) levels (Driscoll, 2003). There is evidence that intrauterine growth restriction occurs in small for gestational age (SGA) newborns, which may be related to the development of PCOS. In a specific cohort of the Brazilian population, the prevalence of PCOS in women who were SGA at birth is twice that in women who had appropriate weight for gestational age (AGA) at birth (Melo et al., 2010). Early onset of puberty and a family history of PCOS are risk factors that must be considered when making this diagnosis in adolescents because the clinical signs are not always evident at this age (Battaglia et al., 2002).
Establishing a diagnosis of PCOS in adolescents is difficult because some symptoms of PCOS in this age group can be confused with normal physiological characteristics of girls this age. During the first years after menarche, 60% of menstrual cycles in girls without PCOS are anovulatory, which is a physiological part of the maturation process (Driscoll, 2003). According to Ehrmann et al. (Ehrmann et al., 1999) menstrual irregularity may be considered to be physiological during the first years after menarche only if there are no associated signs of hyperandrogenism. The PCOS has been discussed in many publications, with difficulty in defining its characteristics. The 2003 Rotterdam consensus workshop (Consesus Rotterdam ESHRE/ASRM, 2004) conclued that PCOS is a syndrome of ovarian dysfunction, and that for its diagnosis two of three criteria might be present. The three criteria established at this consensus are: (1) chronic anovulation characterized by persistent menstrual irregularity for over six months; (2) clinical and/or laboratory hyperandrogenism.
Monitoring adolescents with PCOS is necessary to minimize the clinical and metabolic effects that can interfere with reproductive capacity and progress to chronic degenerative diseases that may increase the risk of morbidity and mortality. The objective of this study was to evaluate predictive factors for MS in adolescent and adult women affected by PCOS.
MATERIAL AND METHODS
A total of 147 consecutive patients from January of 2009 to October of 2010, were recruited at the time of PCOS diagnosis at the Faculty of Medicine of Ribeirão Preto, University of São Paulo (FMRP-USP).
The inclusion criteria used were age (adolescents from 11 to 19 years of age and adult women from 20 to 40 years of age) and a diagnosis of PCOS according to the Rotterdam criteria (Consesus Rotterdam ESHRE/ASRM, 2004), although all patients studied had menstrual irregularities and hyperandrogenism clinical and/or laboratory. The adolescents were at least a period of two years after menarche.
All patients signed an informed consent. The study was approved by the ethics committee through the process HCRP 3505/2009.
Patients were included in the study regardless of race or social status and were divided into two groups: adolescent PCOS (n=42) and adult PCOS (n=105). The exclusion criteria were the presence of any endocrine disease that involves anovulation and/or hyperandrogenism, the use of medications that change the lipid profile, the use of hypertensive and/or hypoglycemic agents, the use of any sex steroids during the three months of the study and pregnancy.
The following data were analyzed for each patient: blood pressure (BP), waist circumference (WC), body mass index (BMI), Ferriman Gallwey index, dehydroepiandrosterone sulfate (DHEAS), 17-hydroxyprogesterone (17-OHP), total testosterone, prolactin, fasting serum insulin, fasting blood glucose, lipid profile (total cholesterol [TC], triglycerides [TG], high density lipoprotein [HDL] and low density lipoprotein [LDL]). All patients received transabdominal pelvic ultrasound (no previous sexual activity) or to transvaginal ultrasound during the follicular phase for the evaluation of the morphological aspect of the ovaries.
After patients fasted for 12 hours, 20 mL of blood was collected. Fasting blood glucose was determined by the oxidase method using the Konelab 60i analyzer by Wiener Lab®, Rosario, Argentina; fasting serum insulin and prolactin were determined by the chemiluminescence method using the DPC 2000 Immulite® analyzer (Diagnostic Products Corporation, Los Angeles, CA, USA); total testosterone, DHEAS and 17-OHP were determined by radioimmunoassay using a Tri-Carb 2100TR liquid scintillation counter (Packard® Instrument Company, IL, USA); TC, HDL and TG were determined by the enzyme method, using the BT 3000 plus apparatus (Wiener lab®) and LDL was calculated using the Friedewald (Friedewald et al., 1972) formula: LDL = TC - (HDL + TG/5). The ultrasound machine used to calculate MOV and for the classification of ovarian micropolycystosis was a Volusom 730 (GE Medical Care, Kretz, Austria), and MOV was calculated using the following formula: MOV = width x depth x length x 0.5 (Griffin et al., 1995).
MS was evaluated according to the criteria of the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) (National Cholesterol Education Program, 2002) modified by Association/National Heart (Grundy et al., 2005), considering for women waist circumference ≥ 88 cm, triglycerides ≥ 150 mg/dl, HDL cholesterol <50 mg/dl, fasting glucose ≥ 100 mg /dl and blood pressure ≥ 130 mmHg or ≥ 85 mmHg, where presence of three criteria define the syndrome diagnosis.
Insulin resistance (IR) was evaluated by the homeostasis model assessment of insulin resistance (HOMA-IR) using the following formula: HOMA = (insulin x 0.055 x blood glucose) / 22.5. Insulin resistance was considered when the value was >2.7 (Geloneze et al, 2009).
Statistical analysis
To verify the normal distribution of quantitative variables, the Kolmogorov-Smirnov and Shapiro-Wilk tests were used. An unpaired t test was used for the comparison of normally distributed data; in the absence of a normal distribution, the Mann-Whitney test was used. The quantitative variables were expressed as mean ± SD. For qualitative variables, the chi-square test or Fisher’s test was used. The significance level was set at 5%.A multiple logistic regression was performed: the dependent variable was the presence of MS and the independent variables were testosterone level, BMI and insulin level. The analysis was performed using SAS software, version 9.0 (SAS Institute, Inc., North Carolina State University, NC, USA).
RESULTS
The mean age of adolescent patients was 16.9 ± 1.5 years, and that of adult patients was 29 ± 4.4 years (p<0.0001). The Ferriman Gallwey scores, testosterone levels, DHEAS, 17-OHP, MOV and BMI were not significantly different between adolescent and adult women. However, WC was greater in adult women than in adolescents (99 ± 16.6 cm vs. 92.9 ± 13.9 cm, p=0.04). Although the systolic blood pressure (SBP) did not differ between the groups, the diastolic blood pressure (DBP) was higher in adult women (79 ± 11 mmHg) than in adolescent women (75.5 ± 6.1 mmHg) (p=0.02). The blood glucose and fasting serum insulin levels were similar for both groups. The HOMA-IR was higher in adult women than in adolescents (2.9 ± 5.3 vs. 0.64 ± 0.67, p<0.0001).
The lipid profile of the adult women was more altered than that of the adolescents. TC and LDL were higher in the adult women (187.8 ± 39.1 mg/dL vs. 163.6 ± 29.4 mg/dL, p=0.001 and 113.6 ± 33.7 mg/dL vs. 90.7 ± 31.6 mg/dL, p<0.0001, respectively). There were no significant differences between the two groups in HDL and TG (Table 1).
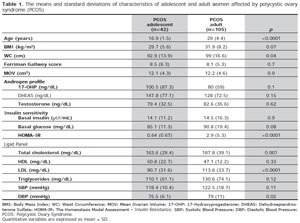
Table 1. The means and standard deviations of characteristics of adolescent and adult women affected by polycystic ovary syndrome (PCOS)
The MS criteria are described in Table 2. In the qualitative analyses, there were no differences between the groups in TG ≥150 mg/dL, HDL <50 mg/dL or blood glucose ≥100 mg/dL. Both MS (49.5% vs. 23.8%, p=0.01), relation to obesity (72% vs. 40.5%, p=0.005) and BP ≥ 130/85 mmHg (42% vs. 16.7%, p=0.026) differed between the adult and adolescent patients with PCOS.
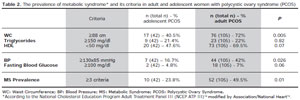
Table 2. The prevalence of metabolic syndrome* and its criteria in adult and adolescent women with polycystic ovary syndrome (PCOS)
In the multivariate analysis for the adult women, insulin level and BMI were independent predictors of MS incidence (p<0.01 for both variables); however, for adolescents, only the BMI independently predicted the incidence of MS (p<0.03; Table 3).
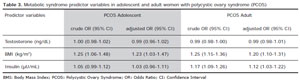
Table 3. Metabolic syndrome predictor variables in adolescent and adult women with polycystic ovary syndrome (PCOS)
DISCUSSION / CONCLUSION
The persistence of anovulatory cycles for more than 24 months after menarche, especially if associated with other characteristic of hormonal disorders, may suggest ovulatory dysfunction of pathologic origin, with hyperandrogenic anovulation being the condition most frequently detected (Avvad et al., 2001). In a study in adolescents in our midst (Fernandes et al., 2005) 14/22 patients with menstrual irregularity had associated clinical signs of hyperandrogenism (Ferriman-Gallway score ≥ 8) suggesting a diagnosis of PCOS. Considering the criteria of PCOS based on the Rotterdam consensus (Consesus Rotterdam ESHRE/ASRM, 2004) they found that 21/22 patients fulfilled the diagnostic. These findings agree with other authors who point to menstrual irregularity as the most precocious marker of PCOS. Based on these data, the present study, all adolescent patients diagnosed with PCOS had irregular menstrual periods.
An important aspect of this cross-sectional study is its simultaneous analysis of the changes that the metabolic repercussions of PCOS may cause in two separate stages of reproductive life at different exposure times.
In the population studied, the presence of obesity and a WC ≥ 88 cm was observed in approximately 40.5% of adolescents with PCOS. The increase in childhood obesity is correlated with an increase in WC, and this parameter is reported to be a good marker of abdominal visceral fat (Coviello et al., 2006). Visceral adiposity, in turn, is associated with IR, a primary pathophysiological mechanism that is responsible for the metabolic disorders of MS. It is important to note that the association of obesity with this syndrome is independent of age, as noted in the literature (Gambineri et al., 2002); this was also observed in this study, with a similar prevalence of obesity in adult and adolescent women with PCOS. This study demonstrated that the typical clinical and laboratory signs of PCOS are present, regardless of age, due to the lack of difference between the groups in androgen levels, Ferriman Gallwey index and MOV.
The prevalence of IR in adults with PCOS, as measured by HOMA-IR, was greater than that observed in adolescents, and insulin was an independent predictive variable for the incidence of MS, reflecting its direct effect on metabolic repercussions.
The prevalence of IR may have been underestimated in this study. The best method for IR identification is the euglycemic hyperinsulinemic clamp described by DeFronzo et al. (DeFronzo et al., 1979). This method can be used to accurately assess the rate of whole-body glucose disposal during steady-state hyperinsulinemia. The oral glucose tolerance test (OGTT) has also been used, in addition to several insulin sensitivity indices, to evaluate IR; these methods are less invasive and more cost-effective than the euglycemic hyperinsulinemic clamp. A previous study performed by our group to evaluate IR in women with PCOS showed that the rate of IR detected by insulin sensitivity indices was 44.8 to 51.4%, which is lower than expected when compared to the rate detected by the OGTT (Martins et al., 2007).
As the duration of exposure to PCOS increased over time, there was an emergence of health complications for these women. There was a higher prevalence of risk factors for the development of cardiovascular diseases (BP ≥ 130/85 mmHg and elevated levels of TC and LDL) in adult women than in adolescents. This broader view of PCOS has established a reconfiguration of the syndrome from an endocrine disorder with only reproductive effects to a metabolic syndrome with reproductive implications, a change that has also altered the therapeutic approaches for these women (Norman et al., 2007).
Soares et al. (Soares et al., 2010) found changes in the vascular elasticity of the carotid artery in young women with PCOS, even in the absence of classic risk factors for cardiovascular disease such as arterial hypertension and obesity.
These authors attributed an increase in the arterial stiffness index and reduction in arterial distensibility to the possible role that hyperandrogenism plays in PCOS and not the comorbidities associated with the syndrome. The mechanism responsible for reduced arterial elasticity in PCOS patients has not yet been determined. To evaluate the effects of sex steroids on arterial stiffness, Natoli et al. (Natoli et al., 2005) studied human aortic smooth muscle cells incubated in vitro with different sex steroids. The proportion of elastin/collagen ratio in cells incubated with estradiol and progesterone was 11-fold greater than in cells incubated with testosterone. This reduction of elastin in the presence of testosterone may result in greater arterial stiffness in vivo. Reduced arterial stiffness was also detected in patients with DM2, probably due to deficient non-enzymatic glycation of elastin and collagen in the arterial tunica (Schram et al., 2004). Therefore, according to Soares et al. (Soares et al., 2010), it is reasonable to suggest that this mechanism relates to PCOS due to the greater prevalence of IR and DM2 in these women.
The prevalence of MS in adult women was 49.5%, which is double the value found in adolescent women (23.8%) and is consistent with previous reports. The prevalence of MS in patients with PCOS, according to the NCEP ATP III (National Cholesterol Education Program, 2002) criteria, varies from 33 to 43%, which is approximately 2 to 4 times higher than levels observed in an ageand BMI-matched general population (Ehrmann et al., 2006). In adult patients with PCOS, the prevalence of MS is higher in individuals with a BMI greater than 27 kg/m2 and with increased insulin levels but does not correlate with circulating androgen levels (Apridonidze et al., 2005). In Brazil, there is a high rate of MS in adult women affected by PCOS, with a general prevalence of 28.4%, but the rate is 52.3% in the subgroup of obese women (Soares et al., 2008) Through our multivariate analysis, insulin and BMI were found to be independent predictors of MS in adult women with PCOS, whereas in adolescents with PCOS, only BMI independently predicted MS. Hyperandrogenism was not an independent predictor of MS development in either group of women affected with PCOS. However, in another study, PCOS group was compared to a control group without PCOS, andhyperandrogenism was considered a risk factor for MS in adolescents with PCOS, regardless of obesity, level of IR or sex hormone-binding globulin (SHBG) level (Coviello et al., 2006).Chen et al. (Chen et al., 2007) demonstrated a positive correlation between serum levels of androgens and SBP and DBP values in young women with PCOS, regardless of age or status of IR, obesity or dyslipidemia; nevertheless, the mechanisms by which a hyperandrogenic state causes an increase in blood pressure have still not been fully elucidated. These findings indicate that the relationship between MS and PCOS involves complex mechanisms that depend not only on constitutional factors but also on levels of insulin, androgens and BMI.
Follow-up studies of adolescents with PCOS are needed to assess the impact of the clinical segment of the women on the risk of metabolic complications in adult life A greater appreciation of initial symptomatology is essential to allow for early therapeutic intervention, including behavioral modification, to minimize acute and chronic consequences of this condition.
ACKNOWLEDGEMENTS
This study received financial support from the National Council of Research and Technology Development (CNPq), process no. 136404/2009-0.
Aribi M. Candidate genes implicated in type 1 diabetes susceptibility. Curr Diabetes 2008;4:110-21.
Driscoll DA. Polycystic ovary syndrome in adolescence. Semin Reprod Med 2003;21:301-7.
Norman RJ, Dewailly D, Legro RS, Hickey TE Polycystic ovary syndrome. Lancet 2007;370:685-97.