JBRA Assist. Reprod. 2011;15(1):40-43
ARTIGO DE REVISÃO
doi: 10.5935/1518-0557.2011.15.1.09
Endometriose e fertilização in vitro. Aspectos atuais.
Endometriosis and in Vitro Fertilization. New aspects
1Bióloga, doutoranda do Curso de Ciências da Saúde da Pontifícia Universidade Católica do Paraná, Curitiba, Paraná
2Médica Ginecologista e Obstetra, Professora Adjunta do curso de Medicina e do Programa de Pós-Graduação em Ciências da Saúde da Pontifícia Universidade Católica do Paraná e Professora Adjunta do Departamento de Tocoginecologia da Universidade Federal do Paraná
RESUMO
Endometriose é uma afecção benigna e caracterizada por uma alta taxa de recorrência. A sua etiologia e patogenêse permanecem ainda indefinidos. Tipicamente, a endometriose causa dor e infertilidade, apesar de até 20-25% das pacientes serem assintomáticas. O tratamento cirúrgico é realizado pela videolaparoscopia com a exerese dos implantes de endometriose. A associação de tratamento médico clínico ou cirúrgico multiprofissional favorecem a qualidade de vida de mulheres com endometriose . Apesar desta vantagem teórica , não existe evidência de que a combinação do tratamento médico cirúrgico melhore significativamente a fertilidade, e podendo desnecessariamente atrasar os tratamentos especializados . O propósito desta revisão é avaliar se os métodos de tratamento da endometriose podem favorecer os resultados dos programas de Fertilização in Vitro e como a endometriose pode afetar o números de oócitos, a qualidade embrionária e a possibilidade de gravidez.
Palavras-chave: endometriose, infertilidade, fertilização in vitro, qualidade embrionária, implantação.
ABSTRACT
Endometriosis is a benign condition characterized by high recurrence rates. The etiology and pathogenesis remain unclear. Typically, endometriosis causes pain and infertility, although 20-25% of patients are asymptomatic.Surgical treatment aims of therapy include relief of symptoms, resolution of existing endometriotic implants.Specific combinations of multiprofessional approach can ameliorate the quality of life of women with endometriosis. Although theoretically advantageous, there is no evidence that a combination medical-surgical treatment significantly enhances fertility, and it may unnecessarily delay further fertility therapy . The purpose of the review was to explore how the endometriosis’s treatments can improve the performance of In Vitro Fertilization programs, how the endometriosis affects the oocytes numbers , embryos quality and pregnancy outcome .
Key-words: endometriosis, infertility, in vitro fertilization, embryo quality, implantation.
Endometriosis is a very common debilitating disease that occurs in 6 to 10% of the general female population; in women with pain, infertility, or both, the frequency is 35- 50%. ( Bullett , C et al ,2010a) Women with endometriosis typically present with pelvic pain, infertility or an adnexal mass. Surgical or medical therapy is efficacious for pelvic pain due to endometriosis, but treatment of endometriosis in the female partner of an infertile couple raises a number of complex clinical questions that do not have simple answers. There are few infertility problems requiring greater clinical acumen than those needed to plan therapy for an infertile woman with endometriosis. (The Practice Committee of the American Society for Reproductive Medicine, 2004)
Fecundity is defined as the probability of a woman achieving a live birth for any given month . In normal couples, fecundity is in the range of 0.15 to 0.20 per month and decreases with age . In untreated women with endometriosis and infertility, monthly fecundity is 0.02 to 0.10. Early studies suggested that 25% to 50% of infertile women have endometriosis and that 30% to 50% of women with endometriosis are infertile. There is a higher prevalence of endometriosis in infertile women (48%) compared with fertile women undergoing tubal sterilization (5%). Others reports have confirmed that infertile women are 6 to 8 times more likely to have endometriosis than fertile women.
The hypothesis that endometriosis causes infertility or a decrease in fecundity remains controversial. Whereas there is a reasonable body of evidence to demonstrate an association between endometriosis and infertility, a cause and effect relationship has not been established.
On the premise that endometriosis does cause infertility, then eradication of the disease should improve fecundity. Two randomized controlled trials (RCTs) have compared outcomes following laparoscopic ablation or expectant management of endometriosis. In the Canadian Collaborative Group on Endometriosis RCT involving 341 women with stage I/II disease followed for 36 weeks after laparoscopy, monthly fecundity was 0.047 and 0.024 in the ablated and untreated groups, respectively .
In the Gruppo Italiano per lo Studio dell’ Endometriosi RCT involving 101 women with stage I/II disease followed for 52 weeks after laparoscopy, fecundity was 0.016 and 0.019 in the ablated and untreated groups, respectively . Although fecundity was significantly improved only in the Canadian surgical trial, fecundity remained significantly lower than that observed in normal fertile women. Thus the visible lesions of endometriosis contribute only a small fraction of the reduced fecundity seen in women with endometriosis.( Parazinni,F 1999)
There are several biologic mechanisms that may link endometriosis and infertility , none of these mechanisms has been proven to decrease fecundity in women . These mechanisms are: distorted pelvic anatomy , altered peritoneal function , altered hormonal and cell - mediated function , endocrine and ovulatory abnormalities and impaired implantation.( Schenken, RS 1984 , Sunigani et al 1988 , Lebovic et al 2001)) Whereas medical therapy is effective for relieving pain associated with endometriosis, there is no evidence that medical treatment of endometriosis improves fecundity. Several options have been suggested for treatment: danazol, gonadotropin-releasing hormone agonists (GnRH-a) and antagonists, progestins and combined estrogen-progestin therapy. In stage I/II endometriosis, laparoscopic ablation of endometrial implants has been associated with a small but significant improvement in live birth rates. Stage III/ IV endometriosis, without other identifiable infertility factors, conservative surgical treatment with laparoscopy and possible laparotomy may increase fertility .( Bullet , C et al 2010b)
More recent data indicate that the incidence of endometriosis has not increased in the last 30 years and remains at 2.37-2.49/1000/y, which equates to an approximate prevalence of 6-8%. A complex network of humoral and cellular immunity factors modulates the growth and inflammatory behavior of ectopic endometrial implants and affects embryo implantation.( Bulleti , C et al 2010c) Women with endometriosis have an increased volume of peritoneal fluid with a high concentration of activated macrophages, prostaglandins, IL-1, TNF, and proteases. These alterations may have adverse effects on the function of the oocyte, sperm, embryo, or fallopian tube. Moreover, an ovum capture inhibitor (OCI) in endometriosis peritoneal fluid is thought to be responsible for fimbrial failure of ovum capture
Elevated levels of IgG and IgA antibodies (autoantibodies to endometrial antigens) and lymphocytes may be found in the endometrium of women with endometriosis.
These abnormalities may alter endometrial receptivity and embryo implantation.
Some authors have reported that uterine implantation was affected by changes in receptivity in endometriosis. Uterine contractility (UC) controls the processes of endometrial shedding at the time of menstruation, transport of gametes, conception, implantation, and maintenance of ongoing pregnancies . Abnormal UC patterns are mainly associated with three medical entities: dysmenorrhea , endometriosis , and infertility . Endometriosis and the presence of endometrial cells in the abdomen were recently related to a specific pattern of UC . (Bulleti, C et al 2010d)
The surgical removal of endometriotic implants in minimal-mild severity endometriosis was shown to improve fertility in two randomized controlled studies IVF-ET is particularly appropriate in cases of infertility associated with a history of endometriosis that involve compromised tubal function, male factor, and/or other treatment failures . In particular, IVF-ET is a powerful therapeutic tool for the treatment of infertility-related endometriosis after failure of other lines of treatment.
Aboulghar suggested that, when the objective is to treat infertility, IVF-ET without prior surgery would probably be the best option. Thus, patients with a diagnosis of advanced endometriosis may be encouraged to undergo IVF-ET as the first-line treatment, before any attempt at surgical treatment (Aboulghar, MA et al 2003).
Despite some evidence showing lower pregnancy rates with IVF in patients with endometriosis compared to patients with other indications for IVF , IVF can be an effective treatment for infertility associated with endometriosis . Surgical removal of endometriosis lesions and adhesions has been shown to improve monthly fecundity rates in women attempting to conceive spontaneously. In addition, we have found in an earlier study higher pregnancy rates in patients who had surgical treatment of endometriosis after a failed IVF attempt compared to those without surgery Barnhart et al (2002) included data from 22 studies, for a total of 2,377 IVF cycles of women with endometriosis cycles and of 4,383 IVF cycles of women without endometriosis. Table I summarizes all the studies and the results concerning the impact of endometriosis in the IVF treatment . The finding of a negative association of endometriosis and a lower pregnancy rate was consistent in all analyses. The meta analysis noted a statistically significant negative association in the crude analysis and a stronger negative association after controlling for confounding variables. Additionally, was demonstrated a poorer success with IVF with an increase in severity of the disease. There is a 36% reduction in pregnancy rate for those with severe endometriosis compared with those with mild disease (OR, 0.64; CI, 0.35-1.17).
These data therefore suggest that the presence of endometriosis affects multiple aspects of the reproductive cycle, including oocyte quality, embryogenesis, and/or the receptivity of the endometrium. ( Barnhart , K et al 2002) Suzuki et al., 2004 made a retrospective study with 611 cycles divided in three goups : Group A (n=80cycles) had ovarian endometriomas that were aspirated and identified as “chocolate” cysts at the time of oocyte retrieval , Group B (n=248 cycles) was the endometriosis diagnosed by laparoscopic before IVF cycle and Goup C ( n=283 cycles) undergoing IVF because of tubal factor without endometriosis previously diagnosed by laparoscopy.
These groups were compared for differences in retrieved number of oocytes, fertilization rate, embryo quality, implantation rate, pregnancy rate, and live birth rate.
Even after two decades of IVF-ET treatment, IVF outcomes in patients with endometriosis remain controversial. Table II shows the results between the three groups.
Some investigators have found no differences in pregnancy rates when comparing patients with and without endometriosis (Diaz , I et al 2000). Alternatively, adverse effects of endometriosis on oocyte and embryo quality, as well as on implantation rates, have been reported by several investigators . Barnhart et al. recently performed a meta-analysis on the effects of endometriosis on IVF; they found that the “pregnancy rate is almost one-half that of women with other indications for IVF” and that “the effect of endometriosis is not exclusively on the receptivity of the endometrium but also on the development of the oocyte and embryo” . In Suzuki’s study, significantly fewer oocytes were retrieved from the endometriosis groups (group A and group B) than from the nonendometriosis group (group C). Although the fertilization rate was slightly, but not significantly, lower in the endometriosis groups (group A and group B), the depressive effects of endometriosis on oocyte development are consistent with the meta-analysis.
The results from Suzuki’s retrospective study suggest that endometriosis does not affect embryo quality and the related parameters of pregnancy, as indicated by the fertilization rate, embryo quality, implantation rate, pregnancy rate, and live birth rate, independent of an ovarian endometrioma. However, these results also demonstrate that endometriosis, even after diagnostic laparoscopy with treatment when necessary, clearly affects the number of oocytes, irrespective of the presence of an ovarian endometrioma.
Shahine et al.,2009a hypothesize that surgical removal of endometriosis lesions may result in improved embryo quality and if this is true, it may partially explain the higher pregnancy rates observed after surgery for endometriosis in some patients , comparing embryo quality in the same patients undergoing IVF cycles before and after surgical treatment of endometriosis to examine whether or not sugery alters embryo quality in patients with endometriosis - related infertility.
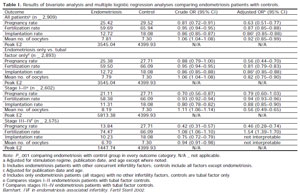
Table I. Results of bivariate analysis and multiple logistic regression analyses comparing endometriosis patients with controls.
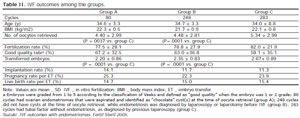
Table II. IVF outcomes among the groups.
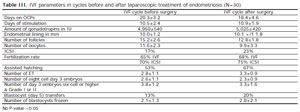
Table III. IVF parameters in cycles before and after laparoscopic treatment of endometriosis (N=30)
Cycles with donor oocytes, preimplanatation genetic diagnosis, and frozen embryo transfer were excluded. All patients had the same male partner during treatment in this time period. Embryos were examined for cleavage (cell number) and grade, which includes cytoplastmic fragmentation. Embryos were graded as follows on day 3: Grade 1, blastomeres have equal size and no cytoplasmic fragmentation; Grade 2, blastomeres have equal size and minor cytoplasmic fragmentation involving < 10% of the embryo;
Grade 3, blastomeres have unequal size and fragmentation involving 10-20% of the embryo; Grade 4, blastomeres have equal or unequal size, and moderate to significant cytoplasmic fragmentation covering 20-50% of the embryo; and Grade 5, few blastomeres and severe fragmentation covering =50% of the embryo ( Shahine et al 2009b). The embryo quality was similar before and after surgical treatment of endometriosis.
The average number of eight cell embryos and good quality embryos (defined as six cell or more and grade I or II) was not significantly different (Table III). A similar percentage of patients met criteria for and underwent blastocyst transfer in the cycles before and after surgery. There was no significant difference in good quality (3BB or better) blastocysts transferred on day 5 in the cycles before surgery compared to those after surgery .(Shahine et al, 2009c)
The live birth rate per IVF cycle after surgical treatment of endometriosis was 43%.
The average time between surgery and retrieval date for IVF cycle after surgery was 211 days in patients that conceived compared to 263 days in those that did not (P=0.4). Live birth rate was 53% for patients with Stage I-II endometriosis and 31% for those with Stage III-IV endometriosis with the second IVF cycle. As the embryo quality appears similar in both cycles, the mechanism for the higher pregnancy rate after surgery may be related to an improved environment for implantation.(Shahine et al 2009d)
The clinical management of an infertile couple should take into account the age of the female, duration of infertility, male factor, duration of medical attention, pelvic pain, stage of endometriosis, and family history. In the management of infertility associated with endometriosis, clinical decisions are difficult because few Randomized Controlled Trials have been conducted to evaluate and compare the effectiveness of the various forms of treatment . Effective, evidence-based treatments of endometriosis-associated infertility include conservative surgical therapy and assisted reproductive technologies.
Patients with endometriosis who are interested in fertility may gain limited benefits with medical therapy. Although theoretically advantageous, there is no evidence that the combination of medical and surgical treatments can significantly enhance fertility, and it may unnecessarily delay further fertility therapy.
Without clear understanding of how endometriosis fully affects fertility, it is difficult to conclude how treatment with IVF or surgery improves pregnancy rates in patients with endometriosis-related infertility.