JBRA Assist. Reprod. 2025;29(4):764-782
REVIEW
doi: 10.5935/1518-0557.20250163
Lead exposure is associated with increased lead bioaccumulation and a decline in semen quality: a systematic review and meta-analysis
1Department of Physiology, Ladoke Akintola University of Technology, Ogbomoso, Oyo State, Nigeria
2Reproductive Biology and Toxicology Research Laboratory, Oasis of Grace Hospital, Osogbo, Osun State, Nigeria
3Department of Agronomy, Osun State University, Ejigbo, Osun State, Nigeria
4Department of Biochemistry, Ahmadu Bello University, Zaria, Kaduna State, Nigeria
5Department of Physiology, Babcock University, Ilishan Remo, Ogun State, Nigeria
6Regions Hospital, Enugu, Enugu State, Nigeria
7Department of Curriculum and Instruction (Science Education), University of Wyoming, USA
8Department of Biological Sciences, Northern Arizona University, Flagstaff, AZ, USA
9Department of Biochemistry, Dokuz Eylul University, Izmir, Turkey
10Department of Community Health, Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria
11Cardiovascular Regenerative Medicine & Tissue Engineering 3D Lab, Department of Cardiovascular Surgery and Research Group for Experimental Surgery, Heinrich Heine University, Medical Faculty, Düsseldorf, Germany
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare
ABSTRACT
Objective: This systematic review and meta-analysis aimed to assess the impact and associated mechanisms of lead on human semen quality.
Methods: A systematic search was conducted from March 18th to April 30th, 2024, utilizing Google Scholar, PubMed, and Scopus, and applying the PECOS model to identify relevant studies.
Results: A total of seventeen studies fulfilled the inclusion criteria. The results of our analysis indicated that blood lead levels were markedly elevated in men exposed to lead compared to control subjects (SMD -7.06 [95% CI: -9.03, -5.08], p<0.00001), with analogous results observed for semen lead levels (SMD -3.42 [95% CI: -5.22, -1.62], p=0.0002). Lead exposure was linked to significant decreases in ejaculate volume (SMD 0.81 [95% CI: 0.16, 1.45], p=0.02), sperm count (SMD 2.10 [95% CI: 1.11, 3.09], p<0.0001), sperm concentration (SMD 0.77 [95% CI: 0.09, 1.44], p=0.03), and total motility (SMD 2.20 [95% CI: 1.28, 3.11], p<0.00001), as well as an increase in abnormal sperm morphology (SMD -3.29 [95% CI: -4.87, -1.71], p<0.0001). While reductions in testosterone levels and elevations in semen malondialdehyde were noted, these changes did not reach statistical significance.
Conclusions: This study demonstrates that lead exposure is associated with reduced sperm quality. The present findings highlight the urgent need for strategies to reduce lead exposure and emphasize the importance of further research into potential mitigating interventions.
Keywords: endocrine disruptors, heavy metals, lead, male infertility, semen, testosterone
INTRODUCTION
Lead, a widespread environmental contaminant, poses significant risks to human health. Although its adverse effects, such as adverse effects on the nervous system and heart, are widely recognized, its impact on male reproductive health has received increasing attention. Sources of lead exposure include environmental and occupational, smoking, and lead-containing cosmetics, jewelry, and diets such as root vegetables (Lasisi-Sholola et al., 2024). Due to its widespread use in industrial activities and consumer products (Besong et al., 2023a; 2023b; Farag et al., 2024), exposure to lead is unavoidable. Its ubiquitous presence in the environment raises significant public health concerns regarding the potential for reduced sperm quality in affected communities. According to the World Health Organization (WHO), lead exposure contributes significantly to the global burden of disease, including 2.5% of ischemic heart disease cases, 2.4% of stroke cases, and 12.4% of unexplained cognitive developmental disorders cases (WHO - World Health Organization, 2024).
Lead-induced toxicity stems from its capacity to accumulate within male reproductive organs, such as the testes and epididymis, where it interferes with normal physiological functions (Besong et al., 2024). Lead induces oxidative stress by generating reactive oxygen species (ROS) (Obiwulu, 2019) and undermines antioxidant defenses, resulting in cellular and molecular damage (Besong et al., 2023a; 2023b; 2024). These processes can adversely affect sperm production and quality, as demonstrated by decreased sperm count, motility, and normal morphology (Balali-Mood et al., 2021) and lower testosterone levels (Bentaiba et al., 2023); thus contributing to a decrease in male fertility. However, the precise mechanisms through which lead exposure influences semen quality, including the roles of bioaccumulation, hormone disruption, and oxidative stress, remain inadequately understood.
A significant knowledge deficit exists in the comprehensive elucidation of these mechanisms and the magnitude of the impact of lead on male reproductive health. Previous research has offered fragmented insights, often constrained by methodological limitations and a narrow focus. Notably, the meta-analysis by Giulioni et al. (2023) demonstrated the impact of lead exposure on semen quality; however, the study had some limitations. The number of studies included in the meta-analysis of Giulioni et al. (2023) was limited. Also, the quality of evidence and potential biases were not fully explored. Moreover, the quantitative analysis of the interplay between lead-induced oxidative stress and hormonal alterations has not been conducted, leaving a void in comprehension regarding the broader implications for reproductive toxicity.
To bridge this gap, the current study endeavors to undertake a systematic review and meta-analysis of the literature concerning lead exposure and semen quality. By aggregating data from a diverse array of studies, this research aims to provide a more accurate and generalizable estimation of the impact of lead on male reproductive health. Furthermore, it delves into the underlying mechanisms, including lead bioaccumulation, hormone disruption, and oxidative stress.
MATERIAL AND METHODS
Search strategy and selection of eligible studies
This is a systematic review and meta-analysis that evaluates the harmful effects of lead exposure on the quality of semen. The scientific literature was systematically searched using Google Scholar, Scopus, and PubMed, between March 18, 2024, and April 30, 2024. These Medical Subject Headings and Boolean operators were used: (male infertility OR male reproductive toxicity OR sperm OR semen) AND (lead OR lead exposure OR Pb). All relevant data were harvested without date and language restrictions.
The Population Exposure Comparison Outcome Study Design (PECOS) model was employed to design the inclusion and exclusion criteria, which were used to screen and identify eligible studies.
Population (P): The study population was men in their reproductive age.
Exposure (E): The studied subjects must have been exposed to lead.
Comparison (C): The lead-exposed population must have been compared with an unexposed population/control. In cases where there were no strict controls, the blood concentrations of lead were used to determine the exposure levels.
Outcome (O): The primary outcomes were ejaculate volume, semen viscosity, sperm count, concentration, morphology (normal and abnormal), vitality, and motility (total and progressive), while the secondary outcomes were blood and semen concentrations of lead, serum FSH, LH, and testosterone levels, and semen malondialdehyde (MDA) concentration.
Study design (S): Observational studies in humans.
Published articles were collected by all authors, while three authors (AVI, ACA, and ATM) independently screened the collected studies for eligibility, and discrepancies were resolved by a fourth author (ARE).
Appraisal of the quality of the eligible studies and data collation
Two authors (APJ and ATM) independently assessed the eligibility for studies for risk of bias (RoB) and confidence of certainty. A third author (ARE) resolved all discrepancies. The ErasmusAGE quality score for systematic reviews was used to assess the level of evidence in the included papers (Hamed et al., 2023), while the Newcastle-Ottawa Quality Assessment Form for Cohort Studies was used to assess the RoB (Wells et al., 2025), and the degree of confidence in the evidence was established by the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group recommendations (GRADE, 2014).
Meta-analysis
Quantitative analyses were done using Review Manager (5.4.1). The standardized mean difference (SMD) and 95% confidence interval (CI) were pooled from the included studies. When there was insignificant variation, a fixed effect (FE) model was employed; otherwise, a random effect (RE) model was used. Significant variation exists when the p-value of heterogeneity ≤0.1 or I2≥50%, and it is not significant when the p-value of heterogeneity >0.1 or I2<50%. A statistically significant result was defined as an overall effect value of p<0.05. Sensitivity analyses were performed by removing the research with the highest weight and studies with poor evidence quality (<5), high RoB, and low or very low certainty of evidence to analytically assess the robustness of our findings, detect the potential sources of bias, and improve the reliability of the synthesized evidence. Publication bias was examined visually using the funnel plot.
RESULTS
Study selection and characteristics of the eligible studies
The flow chart showing the search strategy and identification of studies eligible for inclusion is presented in Figure 1. The systematic literature search yielded 4325 papers with an additional 96 identified from the reference lists. After excluding duplicates, irrelevant studies, retracted papers, animal studies, studies in females, and reviews, editorials, case reports, and commentaries, 18 studies from 17 papers were deemed eligible for inclusion.

Figure 1. PRISMA flow chart showing the search strategy and identification of studies eligible for inclusion.
The qualified studies were published between 1996 and 2024. All the studies were cross-sectional. Table 1 also displays additional details about the qualifying studies, including the nation in which the research was carried out, the size of the study population, participant age, exposure length, and the outcome that was measured.
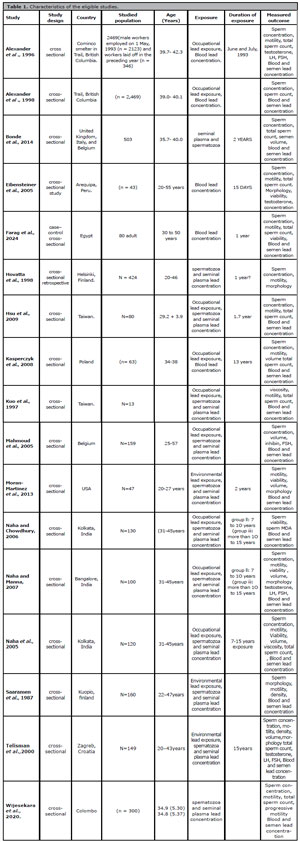
Table 1. Characteristics of the eligible studies.
Study quality
The quality of evidence scores for each domain and the global score are shown in Table 2. All the eligible studies, except Morán-Martínez et al. (2013), showed a good quality of evidence. Two studies (Eibensteiner et al., 2005; Farag et al., 2024) had a marginal quality of evidence. The study design domain had a low score in all the papers since all the eligible studies were cross-sectional.
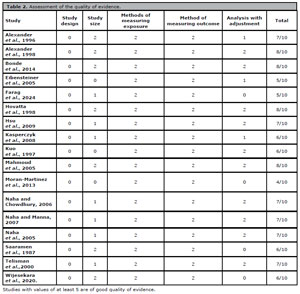
Table 2. Assessment of the quality of evidence.
Table 3 shows the RoB of the included studies. Overall, all studies had a moderate to low RoB. The selection of the exposed cohort and assessment of exposure had a low RoB (1 star) in all the included studies. More so, four studies (Saaranen et al., 1987; Alexander et al., 1996; Kuo et al., 1997; Eibensteiner et al., 2005) had a low certainty of evidence, while ten studies (Alexander et al., 1998; Hovatta et al., 1998; Telisman et al., 2000; Bonde et al., 2002; Mahmoud et al., 2005; Kasperczyk et al., 2008; Hsu et al., 2009; Morán-Martínez et al., 2013; Wijesekara et al., 2020; Farag et al., 2024) had a moderate certainty of evidence, and three studies (Naha et al., 2005; Naha & Chowdhury, 2006; Naha & Manna, 2007) had a high certainty of evidence (Table 4).
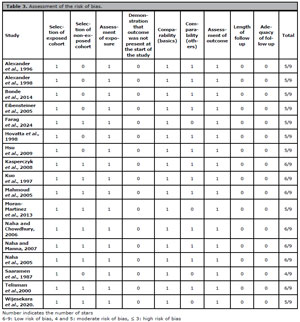
Table 3. Assessment of the risk of bias.
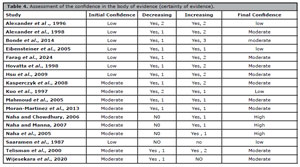
Table 4. Assessment of the confidence in the body of evidence (certainty of evidence).
Quantitative analysis
Lead concentrations in the blood and semen
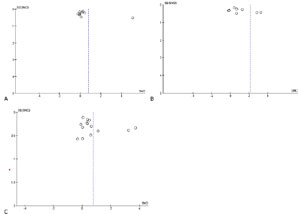
Nine studies were included in the evaluation of blood lead concentration, which included 360 cases of lead-exposed men and 321 controls. Blood lead level was significantly increased in lead-exposed men more than in the control (SMD -7.06 [95% CI: -9.03, -5.08] p<0.00001). The study heterogeneity was significant (I2 = 98%; X2p<0.00001). After sensitivity analysis, the significant difference in blood lead concentration between the control and lead-exposed men persisted (SMD -10.85 [95% CI: -14.49, -7.22] p<0.00001), with a considerable study heterogeneity (I2 = 99%; X2p<0.00001) (Fig. 2A). There was no evidence of publication bias. (Supplementary Fig. 1A).

Figure 2. Effect of lead exposure on blood lead concentration (A) and semen lead concentration (B). Values are shown as standardized mean difference and 95% confidence interval.
Quantitative analysis of the eight studies included in the evaluation of semen lead concentration revealed that exposure to lead led to a significant rise in semen lead levels when compared with the controls (SMD -3.42 [95% CI: -5.22, -1.62] p=0.0002). There was a significant inter-study diversity (I2 = 98%; X2p<0.00001). After sensitivity analysis, semen lead concentration was yet significantly higher in lead-exposed men than in the controls (SMD -6.89 [95% CI: -12.35, -1.44] p=0.01), and there was also a considerable study heterogeneity (I2 = 99%; X2p<0.00001) (Fig. 2B). There was no evidence of publication bias (Supplementary Fig. 1B).
Semen viscosity
The meta-analysis assessing the effect of exposure to lead on semen viscosity only had three studies: 73 control and 45 lead-exposed men. No significant difference was found in the semen viscosity of men exposed to lead when compared with the control group (SMD 1.97 [95% CI: -0.42, 4.37], p=0.11). There was a significant inter-study diversity (I2 = 94%; X2p<0.00001) (Supplementary Fig. 2A). There was a considerable publication bias (Supplementary Fig. 2B).
Ejaculate volume
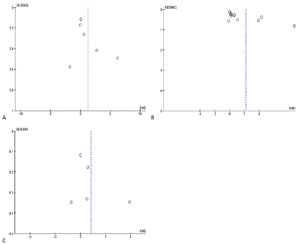
Quantitative analysis of eleven studies (514 control versus 517 lead-exposed) showed that the control subjects had a significantly higher ejaculate volume than the lead-exposed men (SMD 0.81 [95% CI: 0.16, 1.45] p=0.02), with a considerable study heterogeneity (I2 = 95%; X2p<0.00001). After sensitivity analysis, ejaculate volume was still significantly higher in the control than in the lead-exposed men (SMD 1.39 [95% CI: 0.39, 2.38] p=0.006). This showed a significant study heterogeneity (I2 = 96%; X2p<0.00001) (Fig. 3A). There was a noticeable publication bias (Supplementary Fig. 3A).
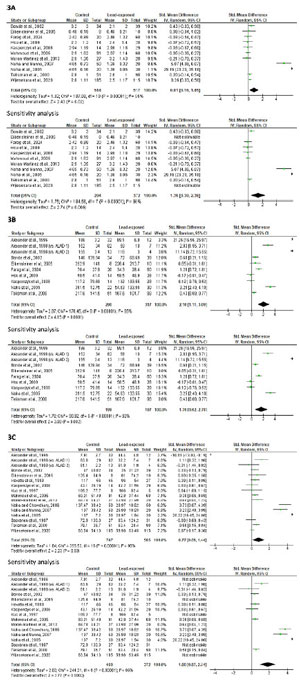
Figure 3. Effect of lead exposure on ejaculate volume (A), sperm count (B), and sperm concentration (C). Values are shown as standardized mean difference and 95% confidence interval.
Sperm count
Meta-analysis of ten studies from nine articles (290 control versus 317 lead-exposed) demonstrated a significantly lower sperm count in lead-exposed men compared with the control (SMD 2.10 [95% CI: 1.11, 3.09], p<0.0001). There was a considerable inter-study diversity (I2 = 95%; X2p<0.00001). After sensitivity analysis, the significant reduction in sperm count following lead exposure persisted (SMD 1.70 [95% CI: 0.62, 2.78], p=0.002). This also revealed a significant study heterogeneity (I2 = 93%; X2p<0.00001) (Fig. 3B). Also, a publication bias was observed (Supplementary Fig. 3B).
Sperm concentration
Quantitative analysis of sixteen studies (747 control versus 565 lead-exposed) showed that lead exposure led to a significantly reduced sperm concentration when compared with the control (SMD 0.77 [95% CI: 0.09, 1.44], p=0.03). There was a substantial heterogeneity (I2 = 96%; X2p<0.00001). More so, a sensitivity analysis of these studies revealed a reduced sperm concentration in lead-exposed men when compared with the control (SMD 1.80 [95% CI: 0.87, 2.74] p=0.0002), with a considerable study heterogeneity (I2 = 96%; X2p<0.00001) (Fig. 3C). There was a substantial publication bias (Supplementary Fig. 3C).
Sperm vitality
Meta-analysis of six studies (341 control versus 353 lead-exposed) showed a marginal but not significant decline in sperm vitality in lead-exposed men when compared with the control (SMD 1.28 [95% CI: 0.03, 2.54] p=0.05) with a significant study heterogeneity (I2 = 97%; X2p<0.00001), which persisted following a sensitivity analysis (SMD 2.21 [95% CI: -0.44, 4.85] p=p0.10) with a significant study heterogeneity (I2 = 99%; X2p<0.00001) (Fig. 4A). A publication bias was observed (Supplementary Fig. 4A).
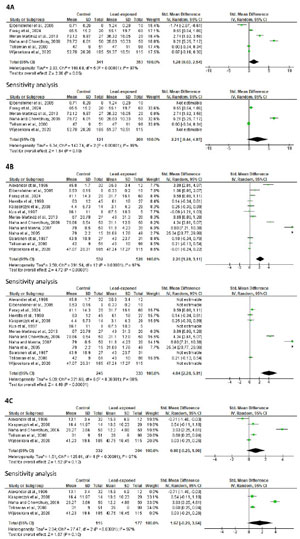
Figure 4. Effect of lead exposure on sperm vitality (A), total motility (B), and progressive motility. Values are shown as standardized mean difference and 95% confidence interval.
Sperm total and progressive motility
Meta-analysis of thirteen studies (532 control versus 526 lead-exposed) showed a significantly lower sperm total motility in lead-exposed men compared with the control (SMD 2.20 [95% CI: 1.28, 3.11] p<0.00001) and a significant study heterogeneity (I2 = 97%; X2p<0.00001). After a sensitivity analysis, sperm total motility was still significantly reduced in lead-exposed men when compared with the control (SMD 4.04 [95% CI: 2.28, 5.81] p<0.00001) and there was a significant inter-study diversity (I2 = 98%; X2p<0.00001) (Fig. 4B). There was a noticeable publication bias (Supplementary Fig. 4B).
Quantitative analysis on sperm progressive motility included five studies which involved 332 control and 304 lead-exposed men. There was no significant alteration in the sperm progressive motility between the control and the lead-exposed groups (SMD 0.86 [95% CI: -0.25, 1.96] p=p0.13) and there was a considerable study heterogeneity (I2 = 97%; X2p<0.00001) even after a sensitivity analysis (SMD 1.67 [95% CI: -0.29, 3.64] p=0.10; I2 = 97%; X2p<0.00001) (Fig. 4C). Publication bias was observed (Supplementary Fig. 4C).
Sperm morphology
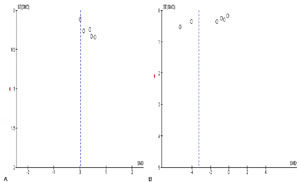
An analysis of six trials comparing 223 men exposed to lead and 311 control men was conducted to determine the effect of lead exposure on normal sperm morphology. Lead exposure did not alter sperm normal morphology (SMD 0.02 [95% CI: -0.51, 0.54] p=0.95), and there was substantial study heterogeneity (I2 = 82%; X2p<0.0001). However, after a sensitivity analysis, lead exposure was observed to significantly reduce sperm normal morphology when compared with the control (SMD 0.40 [95% CI: 0.01, 0.79] p=0.04) and there was no considerable study heterogeneity (I2 = 0%; X2p=0.88) (Fig. 5A). A publication bias was noticed (Supplementary Fig. 5A).

Figure 5. Effect of lead exposure on sperm normal morphology (A) and abnormal morphology (B). Values are shown as standardized mean difference and 95% confidence interval.
Additionally, a meta-analysis of seven studies (232 control versus 302 lead-exposed) demonstrated a significant increase in sperm abnormal morphology in lead-exposed men when compared with the control (SMD -3.29 [95% CI: -4.87, -1.71] p<0.0001) with a significant inter-study diversity (I2 = 98%; X2p<0.00001). After a sensitivity analysis, the observed significant rise in sperm abnormal morphology in men exposed to lead in comparison with the control persisted (SMD -5.00 [95% CI: -7.37, -2.64] p<0.0001) with a significant inter-study diversity (I2 = 97%; X2p<0.00001) (Fig. 5B). Publication bias was observed (Supplementary Fig. 5B).
Hormone profile
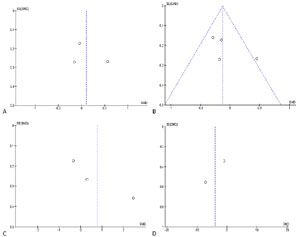
Meta-analysis of the three studies included (137 control versus 140 lead-exposed) revealed that lead exposure did not significantly alter serum LH concentration (SMD 0.10 [95% CI: -0.29, 0.50] p=0.62). There was significant study heterogeneity (I2 = 55%; X2p=0.11) (Fig. 6A). Publication bias was observed (Supplementary Fig. 6A).

Figure 6. Effect of lead exposure on serum LH (A), FSH (B), testosterone (C), and semen MDA concentration (D). Values are shown as standardized mean difference and 95% confidence interval.
In addition, a meta-analysis of four studies (228 control versus 208 lead-exposed) demonstrated that lead exposure did not significantly alter serum FSH levels (SMD -0.13 [95% CI: -0.32, 0.07] p=0.21) and inter-study diversity was not observed (I2 = 48%; X2p=0.12). After a sensitivity analysis, there was yet no significant alteration in serum FSH levels between the lead-exposed and control (SMD 0.12 [95% CI: -0.47, 0.70] p=0.70), and significant inter-study diversity was observed (I2 = 72%; X2p=0.06) (Fig. 6B). Publication bias was also observed (Supplementary Fig. 6B).
Quantitative analysis of three studies (137 control versus 140 lead-exposed) showed no significant difference in serum testosterone concentration in men exposed to lead when compared with the control (SMD 0.78 [95% CI: -0.67, 2.22] p=0.29). There was a significant study heterogeneity (I2 = 96%; X2p=0.29) (Fig. 6C), and publication bias was also observed (Supplementary Fig. 6C).
Semen MDA
Meta-analysis of two studies (64 control versus 79 lead-exposed) revealed that although lead exposure caused a rise in semen MDA level when compared with the control, this was not significant statistically (SMD -4.03 [95% CI: -10.24, 2.19] p=0.20) and a significant study heterogeneity was observed (I2 = 99%; X2p<0.00001) (Fig. 6D). There was no publication bias (Supplementary Fig. 6D).
DISCUSSION
This study not only demonstrated the toxic effect of exposure to lead on semen quality, but it also revealed the involvement of lead bioaccumulation, male reproductive hormones (LH, FSH, and testosterone), and oxidative stress in lead-induced alteration of semen quality. We observed that exposure to lead significantly reduced total motility, normal morphology, ejaculate volume, sperm concentration, and count, but increased abnormal morphology, which was accompanied by a rise in serum and semen lead concentrations.
Findings from this study revealed that lead-induced decline in semen quality may involve several mechanistic pathways. Lead exposure promotes lead accumulation in the serum and semen and may directly induce testicular injury. Lead may disrupt the blood-testis barrier and blood-epididymis barrier, thus promoting its accumulation in these tissues where it impairs spermatogenesis and induces direct injury to germ cells and spermatozoa, leading to reduced total motility, normal morphology, ejaculate volume, sperm concentration, and count. This agrees with the outcomes in experimental studies (Batra et al., 2001; Gorbel et al., 2002) that revealed that lead accumulation disrupts spermatogenesis and damages germ cells.
Although the decline observed in the serum LH and testosterone levels following lead exposure was not statistically significant, it shows that lead exposure may potentially impair testosterone biosynthesis by suppressing the hypothalamic-pituitary axis and/or through the induction of a direct injury to the testis and testicular cells such as the Leydig cells, thus reducing the circulating levels of testosterone. Since optimal levels of testosterone are essential in spermatogenesis (Akhigbe et al., 2024a; Saka et al., 2024), lead-induced suppression of testosterone levels may impair spermatogenesis, which explains the decline in ejaculate volume, sperm count, and concentration.
Furthermore, the marginal rise in MDA levels in the seminal fluid in lead-exposed men is a pointer that lead exposure may trigger oxidative stress, which is initiated by ROS generation and the inactivation of glutathione’s sulfhydryl group that has been connected to lead-induced male reproductive harm (Ommati et al., 2023). Oxidative stress is the result, as this disrupts the oxidant/antioxidant equilibrium, suppressing the antioxidant system and causing a redox imbalance (Famurewa et al., 2023). Lead can cause oxidative stress even though it is not a Fenton reaction heavy metal because it indirectly elevates the level of free ferrous (Fe2+), a Fenton reaction metal that generates hydroxyl radicals and other free radicals (Farinelli et al., 2020). Lead may also cause calcium, copper, and zinc ions to lose their normal functions as membrane signal transducers or cofactors for antioxidant enzymes, hence increasing the creation of ROS from the beginning (Vukelić et al., 2023). Due to the high polyunsaturated fatty acid content, which makes them more susceptible to oxidative damage, the testis and sperm cells are particularly very responsive to lead and its oxidative stress mediators (Vukelić et al., 2023; Akhigbe et al., 2024a). This may, at least in part, explain the observed lead-induced toxicity on semen quality.
The testes and epididymis contain pattern recognition receptors (PRRs) that activate inflammatory pathways in response to excessive ROS. These PRRs may stimulate the development of inflammatory mediators and, in turn, increase ROS production (Dutta et al., 2021). Several experimental studies (Besong et al., 2023a; 2023b; 2024) revealed that lead exposure upregulated pro-inflammatory cytokines like TNF-α and IL-6, suggesting that lead induces inflammatory responses. The oxidative milieu triggered by lead bioaccumulation may also activate NF-κB signaling, promoting the transcription of mRNA transcripts that encode TNF-α and IL-6 (Akhigbe et al., 2024a, 2024b; 2024c). It has been documented that lead-induced reproductive damage is accompanied by oxidative stress, inflammation, and apoptosis. The dual effect of reactive oxygen species (ROS) and/or oxidative stress could accelerate the death of testicular and germ cells (Besong et al., 2023b) by causing cytochrome C to leak into the cytosol (Kolawole et al., 2022).
Available evidence from the literature also reveals that lead toxicity may be mediated by endoplasmic stress (ER)-driven apoptosis and autophagy via the modulation of ER stress-related genes [Glucose regulator protein 78 and 94 (GRP 78, GRP 94), activating transcription factor 4 and 6 (ATF4, and ATF6)] (Rana, 2020). In response to exposure to heavy metals, GRP 78 and immunoglobin protein (BiP), a master ER chaperone, stimulate macrophage activation and control calcium flux and protein folding. ER stress induces apoptosis of spermatocytes by activating the IRE1-JNK/PERK pathway (Kim et al., 2013), thus impairs fertility.
Despite the robustness of this study and the credibility of the evidence synthesized, it has its limitations. First, the presence of significant study heterogeneity might influence our findings. It is likely that the heterogeneity may be due to the study design (all were cross-sectional and observational), varying methods, exposure level and duration, and outcome measurements. Also, the presence of publication bias may lead to distortion of our findings and over-inflation of the impact of lead exposure. Lastly, available data were insufficient to conduct the necessary analysis to explore other relevant mechanisms that have been reported in the literature linking lead exposure with a decline in semen quality. Nonetheless, the strength of this study hinges on several factors. Firstly, it appears that this is the first thorough meta-analysis proving the harmful effects of exposure to lead on semen quality and bioaccumulation, which adds to the mounting evidence of emerging risk factors of male infertility. In addition, the negative impact of the observed study heterogeneity was trimmed by the use of a RE model when a considerable study heterogeneity existed and FE when no study heterogeneity existed. Also, the influence of publication bias was reduced by the performance of a sensitivity analysis, which identified the potential sources of bias and enhanced the reliability of the findings. More so, this study assessed the quality of evidence, RoB, and certainty of confidence in the involved studies. This buttresses the arguments presented in this study. Finally, although not all mechanisms were explored, this study quantitatively assessed the role of lead bioaccumulation, male reproductive hormone disruption, and oxidative stress in lead-induced decline in semen quality (Fig. 7).
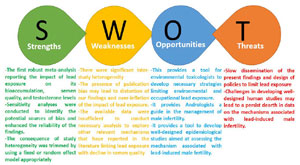
Figure 7. The strengths, weaknesses, opportunities, and threats (SWOT) analysis of the present meta-analysis.
Summarily, this study demonstrates that lead exposure significantly reduces ejaculate volume, sperm concentration, total motility, count, and normal morphology but increases abnormal morphology, which is mediated by increased lead bioaccumulation. Thus, necessary strategies to limit environmental and occupational lead exposure should be promoted. In addition, experimental and clinical studies investigating possible interventions that may limit lead bioaccumulation are recommended.
AUTHORS’ CONTRIBUTIONS
Conceptualization and design: VIA, CAA, TMA, and REA. Data curation: VIA, PJA, CAA, TMA, IAO, and REA. Funding acquisition: TMA and REA. Investigation: VIA, PJA, CAA, TMA, IAO, and REA. Methodology: CAA, TMA, and REA. Project administration: VIA, PJA, CAA, TMA, ORK, IAO, FBF, AEA, RPO, BAA, BDO, AOA, SAH, SSM, SBA, PAO, VJA, OEA, RIO, AAO, and REA. Supervision: REA. Validation: PJA, CAA, TMA, and REA. Writing-original draft: VIA, CAA, and REA. Writing-review and editing and final approval: VIA, PJA, CAA, TMA, ORK, IAO, FBF, AEA, RPO, BAA, BDO, AOA, SAH, SSM, SBA, PAO, VJA, OEA, RIO, AAO, and REA.

Supplementary Figure 1. Publication bias of the studies on the effect of lead exposure on blood lead concentration (A) and semen lead concentration (B).
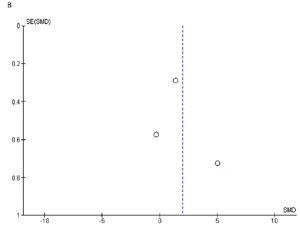
Supplementary Figure 2. Effect of lead exposure on semen viscosity (A) and the publication bias of the studies on semen viscosity (B).
Supplementary Figure 3. Publication bias of the studies on the effect of lead exposure on ejaculate volume (A), sperm count (B), and sperm concentration (C).
Supplementary Figure 4. Publication bias of the studies on the effect of lead exposure on sperm vitality (A), total motility (B), and progressive motility (C).
Supplementary Figure 5. Publication bias of the studies on the effect of lead exposure on sperm normal morphology (A) and abnormal morphology (B).
Supplementary Figure 6. Publication bias of the studies on the effect of lead exposure on serum LH (A), FSH (B), testosterone (C), and semen MDA level (D).
REFERENCES
Akhigbe RE, Adelowo OE, Ajani EO, Oyesetan RI, Oladapo DD, Akhigbe TM. Testicular toxicity in cisplatin-treated Wistar rats is mitigated by Daflon and associated with modulation of Nrf2/HO-1 and TLR4/NF-kB signaling. J Trace Elem Med Biol. 2024a;85:127489. PMID: 38943836 DOI: 10.1016/j.jtemb.2024.127489 Medline
Akhigbe RE, Akhigbe TM, Adegbola CA, Oyedokun PA, Adesoye OB, Adeogun AE. Toxic impacts of arsenic bioaccumulation on urinary arsenic metabolites and semen quality: A systematic and meta-analysis. Ecotoxicol Environ Saf. 2024b;281:116645. PMID: 38941661 DOI: 10.1016/j.ecoenv.2024.116645 Medline
Akhigbe RE, Akhigbe TM, Oyedokun PA, Famurewa AC. Molecular mechanisms underpinning the protection against antiretroviral drug-induced sperm-endocrine aberrations and testicular toxicity: A review. Reprod Toxicol. 2024c;128:108629. PMID: 38825169 DOI: 10.1016/j.reprotox.2024.108629 Medline
Alexander BH, Checkoway H, Costa-Mallen P, Faustman EM, Woods JS, Kelsey KT, van Netten C, Costa LG. Interaction of blood lead and delta-aminolevulinic acid dehydratase genotype on markers of heme synthesis and sperm production in lead smelter workers. Environ Health Perspect. 1998;106:213-6. PMID: 9495797 DOI: 10.1289/ehp.98106213 Medline
Alexander GR, Himes JH, Kaufman RB, Mor J, Kogan M. A United States national reference for fetal growth. Obstet Gynecol. 1996;87:163-8. PMID: 8559516 DOI: 10.1016/0029-7844(95)00386-X Medline
Balali-Mood M, Naseri K, Tahergorabi Z, Khazdair MR, Sadeghi M. Toxic Mechanisms of Five Heavy Metals: Mercury, Lead, Chromium, Cadmium, and Arsenic. Front Pharmacol. 2021;12:643972. PMID: 33927623 DOI: 10.3389/fphar.2021.643972 Medline
Batra N, Nehru B, Bansal MP. Influence of lead and zinc on rat male reproduction at “biochemical and histopathological levels.” J Appl Toxicol. 2001;21:507-12. PMID: 11746199 DOI: 10.1002/jat.796 Medline
Bentaiba K, Belhocine M, Chougrani F, Bououdina M, Mostari A, Fernini M, Bouzouina M. Effectiveness of Withania frutescens root extract on testicular damage induced by lead acetate in adult albino rats. Reprod Toxicol. 2023;115:102-10. PMID: 36535557 DOI: /10.1016/j.reprotox.2022.12.006 Medline
Besong EE, Akhigbe TM, Ashonibare PJ, Oladipo AA, Obimma JN, Hamed MA, Adeyemi DH, Akhigbe RE. Zinc improves sexual performance and erectile function by preventing penile oxidative injury and upregulating circulating testosterone in lead-exposed rats. Redox Rep. 2023a;28:2225675. PMID: 37345699 DOI: 10.1080/13510002.2023.2225675 Medline
Besong EE, Ashonibare PJ, Obembe OO, Folawiyo MA, Adeyemi DH, Hamed MA, Akhigbe TM, Akhigbe RE. Zinc protects against lead-induced testicular damage via modulation of steroidogenic and xanthine oxidase/uric acid/caspase 3-mediated apoptotic signaling in male Wistar rats. Aging Male. 2023b;26:2224428. PMID: 37351853 DOI: 10.1080/13685538.2023.2224428 Medline
Besong EE, Ashonibare PJ, Akhigbe TM, Obimma JN, Akhigbe RE. Sodium acetate abates lead-induced sexual dysfunction by upregulating testosterone-dependent eNOS/NO/cGMP signaling and activating Nrf2/HO-1 in male Wistar rat. Naunyn Schmiedebergs Arch Pharmacol. 2024;397:1233-43. PMID: 37658211 DOI: 10.1007/s00210-023-02696-y Medline
Bonde JP, Joffe M, Apostoli P, Dale A, Kiss P, Spano M, Caruso F, Giwercman A, Bisanti L, Porru S, Vanhoorne M, Comhaire F, Zschiesche W. Sperm count and chromatin structure in men exposed to inorganic lead: lowest adverse effect levels. Occup Environ Med. 2002;59:234-42. PMID: 11934950 DOI: 10.1136/oem.59.4.234 Medline
Dutta S, Sengupta P, Slama P, Roychoudhury S. Oxidative Stress, Testicular Inflammatory Pathways, and Male Reproduction. Int J Mol Sci. 2021;22:10043. PMID: 34576205 DOI: 10.3390/ijms221810043 Medline
Eibensteiner L, Del Carpio Sanz A, Frumkin H, Gonzales C, Gonzales GF. Lead exposure and semen quality among traffic police in Arequipa, Peru. Int J Occup Environ Health. 2005;11:161-6. PMID: 15875892 DOI: 10.1179/oeh.2005.11.2.161 Medline
Farag AGA, Badr EA, Kholif AOA, Khalifa MN, Ghanem MMM. Serum and Seminal Plasma Levels of Lead and Arsenic in Cigarette Smokers and Their Relation to the Semen Parameters. Biol Trace Elem Res. 2024;202:4450-8. PMID: 38180596 DOI: 10.1007/s12011-023-04039-7 Medline
Farinelli G, Minella M, Pazzi M, Giannakis S, Pulgarin C, Vione D, Tiraferri A. Natural iron ligands promote a metal-based oxidation mechanism for the Fenton reaction in water environments. J Hazard Mater. 2020;393:122413. PMID: 32126419 DOI: 10.1016/j.jhazmat.2020.122413 Medline
Giulioni C, Maurizi V, De Stefano V, Polisini G, Teoh JY, Milanese G, Galosi AB, Castellani D. The influence of lead exposure on male semen parameters: A systematic review and meta-analysis. Reprod Toxicol. 2023;118:108387. PMID: 37119974 DOI: 10.1016/j.reprotox.2023.108387 Medline
Gorbel F, Boujelbene M, Makni-Ayadi F, Guermazi F, Croute F, Soleilhavoup JP, el Feki A. Exploration des effets cytotoxiques du plomb sur la fonction sexuelle endocrine et exocrine chez le rat pubère mâle et femelle. Mise en évidence d’une action apoptotique [Cytotoxic effects of lead on the endocrine and exocrine sexual function of pubescent male and female rats. Demonstration of apoptotic activity]. C R Biol. 2002;325:927-40. French. PMID: 12481686 DOI: 10.1016/S1631-0691(02)01492-0 Medline
Hamed MA, Akhigbe TM, Adeogun AE, Adesoye OB, Akhigbe RE. Impact of organophosphate pesticides exposure on human semen parameters and testosterone: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2023;14:1227836. PMID: 37964951 DOI: 10.3389/fendo.2023.1227836 Medline
Hovatta O, Venäläinen ER, Kuusimäki L, Heikkilä J, Hirvi T, Reima I. Aluminium, lead and cadmium concentrations in seminal plasma and spermatozoa, and semen quality in Finnish men. Hum Reprod. 1998;13:115-9. PMID: 9512240 DOI: 10.1093/humrep/13.1.115 Medline
Hsu PC, Chang HY, Guo YL, Liu YC, Shih TS. Effect of smoking on blood lead levels in workers and role of reactive oxygen species in lead-induced sperm chromatin DNA damage. Fertil Steril. 2009;91:1096-103. PMID: 18342860 DOI: 10.1016/j.fertnstert.2008.01.005 Medline
Kasperczyk A, Kasperczyk S, Horak S, Ostałowska A, Grucka-Mamczar E, Romuk E, Olejek A, Birkner E. Assessment of semen function and lipid peroxidation among lead exposed men. Toxicol Appl Pharmacol. 2008;228:378-84. PMID: 18252257 DOI: 10.1016/j.taap.2007.12.024 Medline
Kim JH, Park SJ, Kim TS, Park HJ, Park J, Kim BK, Kim GR, Kim JM, Huang SM, Chae JI, Park CK, Lee DS. Testicular hyperthermia induces Unfolded Protein Response signaling activation in spermatocyte. Biochem Biophys Res Commun. 2013;434:861-6. PMID: 23611781 DOI: 10.1016/j.bbrc.2013.04.032 Medline
Kolawole TA, Asiwe JN, Buduburisi BR, Akintade VA, Adebayo OG, Ojetola AA, Dapper DV. Cabbage (Brassica oleracea) mitigates lead (II) acetate-induced testicular dysfunction in Wistar rats via up-regulation of Bcl-2 protein expression, pituitary-testicular hormonal axis and down-regulation of oxido-inflammatory reactions. Andrologia. 2022;54:e14476. PMID: 35598098 DOI: 10.1111/and.14476 Medline
Kuo HW, Wang CS, Lai JS. Semen quality in workers with long-term lead exposure: a preliminary study in Taiwan. Sci Total Environ. 1997;204:289-92. PMID: 9335162 DOI: 10.1016/S0048-9697(97)00181-2 Medline
Lasisi-Sholola AS, Hammed SO, Ajike RA, Akhigbe RE, Afolabi OA. Estrogen replacement therapy reverses spatial memory loss and pyramidal cell neurodegeneration in the prefrontal cortex of lead-exposed ovariectomized Wistar rats. Curr Res Toxicol. 2024;7:100200. PMID: 39583742 DOI: 10.1016/j.crtox.2024.100200 Medline
Mahmoud A, Kiss P, Vanhoorne M, De Bacquer D, Comhaire F. Is inhibin B involved in the toxic effect of lead on male reproduction? Int J Androl. 2005;28:150-5. PMID: 15910540 DOI: 10.1111/j.1365-2605.2005.00524.x Medline
Morán-Martínez J, Carranza-Rosales P, Morales-Vallarta M, A Heredia-Rojas J, Bassol-Mayagoitia S, Denys Betancourt-Martínez N, M Cerda-Flores R. Chronic environmental exposure to lead affects semen quality in a Mexican men population. Iran J Reprod Med. 2013;11:267-74. PMID: 24639755 Medline
Naha N, Bhar RB, Mukherjee A, Chowdhury AR. Structural alteration of spermatozoa in the persons employed in lead acid battery factory. Indian J Physiol Pharmacol. 2005;49:153-62. PMID: 16170983 Medline
Naha N, Chowdhury AR. Inorganic lead exposure in battery and paint factory: effect on human sperm structure and functional activity. J UOEH. 2006;28:157-71. PMID: 16780224 DOI: 10.7888/juoeh.28.157 Medline
Naha N, Manna B. Mechanism of lead induced effects on human spermatozoa after occupational exposure. Kathmandu Univ Med J (KUMJ). 2007;5:85-94. PMID: 18603992 Medline
Ommati MM, Sabouri S, Retana-Marquez S, Nategh Ahmadi H, Arjmand A, Alidaee S, Mazloomi S, Akhlagh A, Abdoli N, Niknahad H, Jamshidzadeh A, Ma Y, Azarpira N, Asefi Y, Heidari R. Taurine Improves Sperm Mitochondrial Indices, Blunts Oxidative Stress Parameters, and Enhances Steroidogenesis and Kinematics of Sperm in Lead-Exposed Mice. Reprod Sci. 2023;30:1891-910. PMID: 36484981 DOI: 10.1007/s43032-022-01140-5 Medline
Rana SVS. Endoplasmic Reticulum Stress Induced by Toxic Elements-a Review of Recent Developments. Biol Trace Elem Res. 2020;196:10-9. PMID: 31686395 DOI: 10.1007/s12011-019-01903-3 Medline
Saka WA, Adeogun AE, Adisa VI, Olayioye A, Igbayilola YD, Akhigbe RE. L-arginine attenuates dichlorvos-induced testicular toxicity in male Wistar rats by suppressing oxidative stress-dependent activation of caspase 3-mediated apoptosis. Biomed Pharmacother. 2024;178:117136. PMID: 39067166 DOI: 10.1016/j.biopha.2024.117136 Medline
Telisman S, Cvitković P, Jurasović J, Pizent A, Gavella M, Rocić B. Semen quality and reproductive endocrine function in relation to biomarkers of lead, cadmium, zinc, and copper in men. Environ Health Perspect. 2000;108:45-53. PMID: 10620523 DOI: 10.1289/ehp.0010845 Medline
Vukelić D, Djordjevic AB, Anđelković M, Antonijević Miljaković E, Baralić K, Živančević K, Bulat P, Radovanović J, Đukić-Ćosić D, Antonijević B, Bulat Z. Subacute Exposure to Low Pb Doses Promotes Oxidative Stress in the Kidneys and Copper Disturbances in the Liver of Male Rats. Toxics. 2023;11:256. PMID: 36977021 DOI: 10.3390/toxics11030256 Medline
Wijesekara GUS, Fernando DMS, Wijeratne S. The effects of Pb on sperm parameters and sperm DNA fragmentation of men investigated for infertility. J Basic Clin Physiol Pharmacol. 2020;31:20190239. PMID: 32374284 DOI: 10.1515/jbcpp-2019-0239 Medline