JBRA Assist. Reprod 2006;10(4):34-39
ARTIGO DE REVISÃO
doi: 10.5935/1518-0557.2006.10.4.07
A Systematic Review on the Use of GnRH Agonists and Antagonists in Patients with Poor Response to Ovarian Stimulation Supression
Uma Revisão Sistemática Sobre o uso de Agonistas e Antagonistas do GnRH em Pacientes Más Respondedoras à Estimulação Ovariana
1Centro de Reprodução Humana Prof. Franco Junior, Ribeirão Preto, SP
2Pós-graduanda, Departamento de Ginecologia e Obstetrícia, Faculdade de Medicina de Botucatu, UNESP, Botucatu, SP
3Faculdade de Medicina da Universidade de Santo Amaro, São Paulo, SP
ABSTRACT
The purpose of this investigation was to make a systematic review of the medical literature in order to compare the efficacy of GnRH antagonists and agonists for poor responders to ovarian stimulation. According to the data collected, the use of GnRH antagonist protocols showed better results in comparison to long protocols with a GnRH agonist regarding the following aspects: lower cycle cancellation rate due to poor ovarian response; higher number of oocytes retrieved; higher clinical pregnancy rate per initiated cycle.Nevertheless, these results were not observed when the flare-up protocols of GnRH agonists were used. Moreover the number of oocytes retrieved with GnRH agonist was significantly higher in relation to the GnRH antagonist.
Keywords: poor responders, ovarian stimulation, GnRH agonist, GnRH antagonist
RESUMO
A presente investigação teve como objetivo fazer uma revisão sistemática da literatura médica visando comparar a eficácia de agonistas e antagonistas do GnRH em más respondedoras à estimulação ovariana. Os dados de literatura mostraram melhores resultados com os protocolos de antagonistas do GnRH, em comparação com GnRH agonistas aplicados na 2ª fase do ciclo menstrual (protocolo longo), no que se refere aos seguintes aspectos: menor taxa de cancelamento de ciclos por má resposta ovariana; maior número de oócitos coletados; maior taxa de gravidez por ciclo iniciado.Entretanto, essas vantagens não foram observadas quando os agonistas do GnRH foram utilizados com o protocolo de “flare-up”. Além disso, o número de oócitos coletados nos protcolos com GnRH agonista “flare-up” foi significativamente superior aos obtidos com GnRH antagonistas.
Unitermos: más respondedoras, estimulação ovariana, agonistas do GnRH, antagonistas do GnRH.
INTRODUCTION
Recruitment and development of multiple follicles in response to ovarian stimulation are the key factors leading to successful treatment by IVF/ICSI and embryo transfer. Garcia et al. (1983) first described as a poor responder the patient with peak estradiol levels <300 pg/ml and a decreased follicular response, expressed as fewer retrieved and fertilized oocytes and also fewer transferred embryos.
Poor ovarian response, on the other hand, is usually associated with poor pregnancy rates and many of these cycles are cancelled without proceeding to egg collection (Keay et al., 1997). Several strategies have been suggested to prevent cycle cancellation, such as decreasing the dosage and timing of gonadotrophin-releasing hormone agonists (GnRH-a) (Scott and Navot, 1994) or the use of GnRH-a flare-up regimens (Surrey et al., 1998). This procedures should theoretically eliminate excessive ovarian suppression while taking advantage of the additional gonadotrophin stimulus provided by the ago nistic effect of the GnRH-a.
The introduction of GnRH antagonists into clinical practice might be a new hope for poor responder patients (Craft et al., 1999). GnRH antagonists act promptly and only a few hours of administration are required to prevent the LH surge, which is the most common cause for cancellation in poor responder patients. The action of the GnRH antagonist does not result in early folliculogenesis inhibition, which is a critical point for patients with a limited cohort of follicles (Akman et al. 2000, 2001).
The objective of this review is to compare the efficacy of GnRH antagonist to that of a GnRH agonist as coadjuvant medicine for protocols of ovarian hyperstimulation in poor ovarian responder patients in IVF/ICSI cycles.
MATERIALS AND METHODS
Criteria for considering studies for this review
All published, unpublished and ongoing randomized controlled trials (RCT) comparing a GnRH antagonist with GnRH-a in ovarian hyperstimulation protocols for poor responders were analyzed.
Types of outcome measures
The primary outcome measures used for this systematic review were cycle cancellation rate (CCR) due to poor response and the number of retrieved and mature oocytes. The secondary outcomes were clinical pregnancy rate (CPR) per cycle initiated, CPR per oocyte retrieval and CPR per transfer.
Identification of studies
Search strategies included on-line surveys of databases (ME- DLINE, EMBASE, Science Citation Index, Cochrane Controlled Trials Register and OVID) from 1990 to 2006. There was no language restriction and grey literature was included (BiomedCentral, Gateway, TrialsCentral, OMNI, etc.). The following Medical Subject Headings and text words were used: “poor responder”, “ovarian stimulation”, “GnRH antagonist”, “GnRH agonist” and “randomized controlled trial”. The principal inclusion criterion was randomized controlled trial.
Validity assessment and data extraction
Each trial was assessed independently by two reviewers and ranked for its methodology rigor and its potential to introduce bias. Missing data were obtained from the authors when possible.
Statistical analysis
Data management and analysis were conducted using the StatsDirect statistical software (Cheshire, UK). Effectiveness was evaluated using the Mantel-Haenszel method. A confidence interval for the Mantel-Haenszel odds ratio in StatsDirect was calculated using the Robins, Breslow and Greenland variance formula. A chi-square test statistic was used with its associated probability that the pooled odds ratio (OR) was equal to one. The StatsDirect also gives the option to base effect size calculations on weighted mean difference (WMD) as described in the Cochrane Collaboration Handbook (Mulrow and Oxman, 1996). The measure of heterogeneity (non-combinability) was evaluated by Cochran’s Q and the Breslow-Day test. A nonsignificant result (i.e. lack of heterogeneity) indicates that no trial has an OR or WMD that is statistically significantly worse or better than the overall common OR or WMD obtained by pooling the data. The fixed effects model was used for odds ratio (OR) and effect size (WMD).
Search results
Six trials fulfilled the inclusion criteria. In all studies, the multiple low-dose (0.25 mg) antagonist regimen was applied (cetrorelix: 4, ganirelix: 2). In 3 trials, a long protocol with a GnRH agonist (leuprolide: 2, buserelin: 1) starting in the midluteal phase of the preceding cycle was used as a reference treatment. In the 3 remaining trials, a flare-up protocol with a GnRH agonist (triptorelin: 1, leuprolide: 2) was used as reference treatment.
RESULTS
Description of the studies included
Akman et al. (2001) conducted a prospective RCT (randomization by consecutive number method) including a total of 48 poor responder patients described from previous cycles (at least two failed IVF attempts) and who presented one of following reasons: baseline follicle stimulating hormone (FSH) concentrations > 15 mIU/ml or estradiol concentration on the day of human chorionic gonadotrophin (HCG) injection <500 pg/ml or less than four mature oocytes retrieved. The patients were divided into two groups: I - 24 patients in 24 cycles in which leuprolide acetate (Lucrin, Abbott, France) at the dose of 40 µg s.c. per day was initiated on cycle day 2 followed by exogenous gonadotrophins (Metrodin HP, Serono Laboratories, Switzerland) on cycle day 3; II - 24 patients in 24 cycles in which ovarian stimulation included a GnRH antagonist (Cetrotide, Asta Medica, Germany), 0.25 mg daily, administered during the late follicular phase.D’Amato et al. (2004) conducted a prospective RCT. The protocols of ovulation induction were randomly assigned to all patients on the basis of the day of the week of their first appointment (Monday and Thursday: long protocol with GnRH analog; Wednesday and Friday: study protocol). The patients were defined as poor responders by their ovarian response (number of mature oocytes retrieved = 3) to a standard long protocol with a GnRH agonist administered for at least two previous IVF/ICSI cycles, when 37% of cycles were canceled because of a weak E2 rise and inadequate follicular growth after a mean FSH dose of 4,750 IU per cycle. Sixty women (group 1) underwent controlled ovarian hyperstimulation with a single dose of leuprolide acetate (Enantone, Takeda, Italy) administered in the midluteal phase. Eighty-five women (group 2) received a GnRH antagonist (Cetrotide, Serono Pharma) in a multidose fashion (2 to 3 ampules per cycle) from the time when at least a single follicle of 16 mm in diameter was observed and/or E2 levels exceeded 1000 pg/ml until the time when the follicle reached = 18 mm diameter, when HCG was injected.Malmusi et al. (2005) conducted a prospective RCT (randomization list). The poor responders (no ovarian response when = 300 IU of FSH were administered for = 15 days or low number of oocytes =4) were randomized into two groups. The first group consisted of 30 patients in 30 cycles in which triptorelin, 0.1 mg (Decapeptyl, Ipsen, France) was initiated on the 1st day of menstruation, followed by exogenous gonadotrophins (Gonal-F, Serono, Switzerland) administered from the 2nd day of menstruation. The second group consisted of 25 poor responders (25 cycles) in whom the exogenous gonadotrophins (Gonal-F, Serono, Switzerland) were started on the first day of the menstrual cycle, followed by ganirelix (Orgalutran, Organon, Netherlands), 0.25 mg, administered daily until HCG injection when the leading follicle reached 14 mm in diameter. In each group, all patients initially received 450 IU of recombinant human FSH and the dose was adjusted individually according to the response of the ovaries.Marci et al. (2005) conducted a prospective RCT (randomized 1:1). The poor responders (estradiol concentrations < 600 pg/ml on the day of HCG administration and a number of retrieved oocyte < 3 after a previous standard long protocol with GnRH-a) were divided into two groups. Group A patients (n=30) were stimulated with a standard long protocol using down-regulation with GnRH-a, one injection of 3.75 mg (Enantone, Takeda, Italy), and a subcutaneous injection of recombinant FSH (Gonal-F, Serono, Italy) at a dose of 375 IU daily from day 3 of the next cycle. In group B (n=30), ovarian stimulation started at day 2 with r-FSH at a dose of 375 IU. The GnRH antagonist cetrorelix (Cetrotide, Serono Laboratories, Switzerland), 0.25 mg per day, was then administered when the two lead follicles had reached 14 mm in diameter, irrespective of the day of the cycle, and continued until day of HCG injection.Cheung et al. (2005) The paper reports a prospective, randomized controlled trial (computer-generated random) concealed in opaque envelopes. A research nurse coordinated the randomization process and distribution of medication throughout the treatment cycles. Doctors and embryologists involved in the study were blinded to the treatment allocation. Poor responders were classified as patients who had exhibited a poor ovarian response with < 3 mature follicles on a long GnRH agonist protocol in their previous IVF cycles or those with repeated high basal levels of FSH > 10 IU/l. The patients were randomly allocated to receive a GnRH antagonist or an agonist. All patients received the oral contraceptive pill (Nordette, Wyeth; 30 µg of ethinyl estradiol and 150 µg of levonorgestrel), one tablet daily, for the rest of the cycle for a total of 21 days. The control group (n=32) received a long GnRH-a protocol. Buserelin acetate (Suprecur, Hoechst AG, Germany) nasal spray was given at a daily dose of 600 µg starting at the mid-luteal phase of the preceding cycle, and co-administered during the final week of oral contraception pre-treatment. Buserelin was continued until the day of HCG administration. The study group (n=31) received a fixed multi-dose (0.25 mg daily) GnRH antagonist protocol (Cetrotide, Serono Laboratories, Switzerland) from day 6 of stimulation until the day of HCG.Schmidt et al. (2005) The paper reports a prospective, randomized controlled trial. Computer-generated randomization was used for patient assignment to two treatment protocols at a 1:1 ratio. Sealed envelopes were used for protocol allocation. A poor responder was defined as a woman with serum peak estradiol level = 850 pg/ml and/or = 4 preovulatory follicles = 15 mm in average diameter present on the day of human chorionic gonadotrophin administration during a previous cycle. A total of 48 patients were randomized to one of two groups: ganirelix acetate (group A; n=24) or microdose leuprolide flare-up (group B; n=24). On cycle day 2, patients randomized to group A received 300 IU of recombinant FSH every morning and 150 IU of human menopausal gonadotrophin (hMG) every evening for 5 days. A multidose regimen of ganirelix was used with daily morning injections until, and including, the day of HCG administration. The patients randomized to group B received leuprolide acetate with a regimen of 40 µg SC every 12 hours. The FSH and hMG dosing, monitoring, and individualized dosing adjustments were the same as for group A.
Primary outcome measures
In the 3 trials that had used long protocols of GnRH agonists as a reference treatment, we observed advantages for the GnRH antagonists protocol with respect to lower CCR due to poor ovarian response (p:0.0002; OR 0.29, 95% CI 0.14, 0.57) (Table 1), a higher number of retrieved oocytes (p<0.0001; WMD:1.98, 95% CI 1.56, 2.40) (Table 2) and a higher number of mature oocytes (p<0.0001; WMD:1.58, 95% CI 1.18, 1.97) (Table 3).
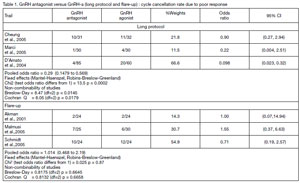
Table 1. GnRH antagonist versus GnRH-a (long protocol and flare-up) : cycle cancellation rate due to poor response
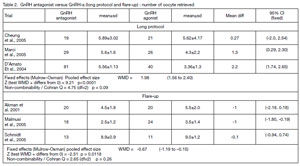
Table 2. GnRH antagonist versus GnRH-a (long protocol and flare-up) : number of oocyte retrieved
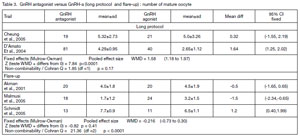
Table 3. GnRH antagonist versus GnRH-a (long protocol and flare-up) : number of mature oocyte
However, when we studied only the 3 trials that had used the flare-up protocol of GnRH agonists as reference treatment, a statistic significantly lower number of retrieved oocytes (p:0.0118; WMD: -0.67, 95% CI -1.19, -0.15) was observed in the GnRH antagonist protocol when compared with the GnRH agonist (Table 2). In addition, no differences were observed regarding CCR due to a poor ovarian response (p:0.87; OR 1.014, 95% CI 0.47, 2.19) (Table 1) or number of mature oocytes (p:0.41; WMD: -0.216, 95% CI -0.73, 0.30) (Table 3).
Secondary outcome measures
In the 3 trials with a long protocol of GnRH agonist as a reference treatment it was observed that the antagonist protocol had higher CPR per initiated cycle (p:0.03; OR 2.34, 95%CI 1.11, 4.94) (Table 4). However, these differences were not observed in the CPR per oocyte retrieval (p:0.14; OR 1.88, 95% CI 0.87, 4.05) or CPR per transfer (p:0.19; OR 1.78, 95% CI 0.82, 3.84).
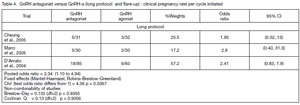
Table 4. GnRH antagonist versus GnRH-a (long protocol and flare-up) : clinical pregnancy rate per cycle initiated
On the other hand, in the 3 trials that used the flare-up protocol of GnRH agonists as reference treatment, no other differences were observed in the GnRH antagonist protocol with respect to secondary outcome measures: CPR per initiated cycle (p:0.80; OR 0.82, 95% CI 0.35, 1.90), CPR per oocyte retrieval (p:0.74; OR 0.78, 95% CI 0.32,1.90), CPR per transfer (p:0.97;OR 0.89, 95% CI 0.27,2.20).
DISCUSSION
Poor ovarian response to gonadotrophin remains a significant problem in assisted conception. There have been various reports formulating the ideal stimulation protocol for poor ovarian responders. It has been documented that cycle cancellation is common for this particular group of patients, mostly due to premature LH surges or to an inadequate ovarian response (Akman et al., 2001).
The lack of a uniform definition of ‘poor responders’ makes it difficult to compare treatment outcomes and develop and assess protocols for prevention and management (Surrery and Schoolcraft, 2000; Kailasam et al., 2004). This fact could be observed in this meta-analyses since the authors used different criteria for the selection of the population defined as poor responder: Akman et al. (2001): FSH, oestradiol and number of mature oocytes; D’Amato et al., 2004: number of mature oocytes and/or FSH dose = 4750 IU with no ovarian response; at least two failures in IVF/ICSI cycles; Malmusi et al. (2005): no ovarian response when =300 IU of FSH were administered for =15 days or low number of oocytes =4; Marci et al. (2005): oestradiol concentrations <600 pg/ml on the day of HCG administration and <3 oocytes retrieved after a previous standard long protocol with GnRHa; Cheung et al.: <3 mature follicles in a long GnRHa protocol in their previous IVF cycles or those with repeated high basal concentrations of FSH >10 IU/l; Schmidt et al. (2005): serum peak oestradiol concentration =850 pg/ml and or =4 preovulatory follicles =15 mm in average diameter present on the day of HCG administration during a previous cycle. An international standardization of criteria to define poor ovarian responders should be an important future measure. This aspect could be a possible limit for the results of this meta-analysis.
In none of the analyzed trials the age was a criterion for patient’s inclusion or exclusion, or even was used as a criterion of poor responder. On the other way, as expected in RCT, in all studies the women ages among the analyzed groups did not present significant statistic difference: Akman et al. 2001: agonist flare-up protocol: mean age: 38 years (28-46) X antagonist protocol: mean age 38.5 years (28-44); D’ Amato et al., 2004: agonist long protocol: mean age 33.02 ± 3.09 years (27-39) X antagonist protocol: mean age 34.01 ± 2.89 years (27-39); Malmusi et al., 2005: agonist flare-up protocol: mean age 36.6.02 ± 0.8 years X antagonist protocol: mean age 36.2 ± 1.2 years; Marci et al., 2005: agonist long protocol: mean age 39.0 ± 3.1 years X antagonist protocol: mean age 38.8 ± 2.9 Years; Cheung et al., 2005 agonist long protocol: mean age 36.3 ± 2.6 years X antagonist protocol: mean age 36.3 ± 3.0 years; Schmidt et al., 2005: all patients were between 25 and 43 years, mean age were similar between the two groups). Despite it was not possible to include the data from all trials in the statistical analysis, the general observation showed differences. However, it should be stressed that trials conducted on diverse populations may better reflect the natural heterogeneity of treatment effectiveness found in daily practice.
The presence of randomization was the primary criterion used to select all the papers of this meta-analysis. An interesting fact observed was the difference among authors with respect to the randomization process (Akman et al. 2001, consecutive number method; D’Amato et al., 2004: days of week; Malmusi et al., 2005: randomization list; Marci et al., 2005: consecutive number method; Cheung et al., 2005: computer-generated randomization; Schmidt et al., 2005: computer-generated randomization). True randomization involves selecting patients by a random process, such as the use of a random-numbers table. Quasi-random methods such as sorting by days of the week, birth dates, or medical record numbers, are reasonable in most cases, although investigators need to test for any bias that might result.
This investigation showed that the use of GnRH antagonist protocols gives better results (a lower CCR due to poor ovarian response, higher number of oocytes retrieved, higher number of mature oocytes retrieved and a higher CPR per initiated cycle) in comparison with long protocols of GnRH-a for controlled ovarian hyperstimulation for poor responders in IVF/ISCI cycles
More recently, with the discovery of extrapituitary GnRH receptors in the human ovary (Janssens et al., 2000), there has been some concern that the non-physiological level of GnRH-a given to achieve down-regulation may have a direct, deleterious effect on the ovary, and contribute to the poor response to ovarian stimulation in some patients undergoing IVF/ICSI cycles. To overcome the extra-suppression hypothesis while preventing the premature LH surges, various researchers have advocated decreasing the dosage and the timing of GnRH-a, such as in microdose GnRH-a agonist and flare-up regimens (Scott and Navot, 1994; Surrey et al., 1998). In this study, the 3 trials with GnRH-a as a reference treatment did not use a microdose regimen.
Tarlatzis et al. (2003) reported that flare-up GnRH-a protocols (including all dosage varieties) produce better results than standard long luteal protocols in patients with poor ovarian response.
In this study, when the review was performed with the trials that had used flare-up protocols of GnRH-a as reference treatment, a statistically significant lower number of retrieved oocytes was observed in the GnRH antagonist protocol when compared with the GnRH agonist. However, no other difference was observed with the GnRH antagonist protocol in any of the outcomes analyzed (CCR due to poor ovarian response, number of mature oocyte, CPR per initiated cycle, CPR per oocyte retrieval, CPR per transfer).
Garcia-Velasco et al (2001) observed that GnRH antagonist therapy in women undergoing ovarian stimulation had a significant effect on ovarian follicular steroidogenesis. The mean estradiol concentration in follicular fluid was significantly lower in patients treated with a GnRH antagonist than in those treated with GnRH-a. In that study, an interesting observation was the fact that, with similar FSH doses (GnRH antagonist and GnRH-a groups) and with a significantly reduced period of stimulation, fewer oocytes were retrieved in antagonist-treated women. However, this was a matching study and not a randomized controlled clinical trial.
Lindheim and Morales (2003) in 37 donor cycles, starting GnRH antagonist administration on day 6 of stimulation, reported that 35% of donor cycles had a decrease in serum estradiol prior to hCG administration and 93% of them showed a decrease in serum estradiol at > 3 days after GnRH antagonist administration. They concluded that the use of GnRH antagonists has an unpredictable effect on estradiol production during follicular recruitment which appears to adversely affect pregnancy outcome if a decline in estradiol occurs.
At present, the relationship between a GnRH antagonist and a negative effect on ovarian follicular steroidogenesis (decreased estradiol levels, low number of oocytes) is unclear. Nevertheless, some variables could be interfering with his problem such as total dose, different length of the downregulation period, and individual sensitivity to the drug.
To our knowledge, this is the first systematic review comparing a GnRH antagonist against GnRH-a in ovarian stimulation protocols for poor responders. Nevertheless, additional randomized controlled trials with better planning are needed to further confirm these results, since the randomized studies available for this meta-analysis involved reduced sample numbers and varied widely in the definition of poor ovarian response, and heterogeneity (trial GnRH-ant versus GnRHa agonist protocols with respect to number of mature oocytes).
Mulrow CD, Oxman AD (eds) - Cochrane Collaboration Handbook, Oxford: Cochrane Collaboration, 1996.